Eye Banking Year in Review – Statistical Report. Eye Bank Association of America. 2021. Available at https://restoresight.org/wp-content/uploads/2022/05/YearInReview_2021_FINAL_HighResolution.pdf.
Tan DT, Dart JK, Holland EJ, Kinoshita S. Corneal transplantation. Lancet. 2012 May 5. 379 (9827):1749-61. [QxMD MEDLINE Link].
Jabbehdari S, Rafii AB, Yazdanpanah G, Hamrah P, Holland EJ, Djalilian AR. Update on the Management of High-Risk Penetrating Keratoplasty. Curr Ophthalmol Rep. 2017 Mar. 5 (1):38-48. [QxMD MEDLINE Link].
Holland G, Pandit A, Sánchez-Abella L, Haiek A, Loinaz I, Dupin D, et al. Artificial Cornea: Past, Current, and Future Directions. Front Med (Lausanne). 2021. 8:770780. [QxMD MEDLINE Link].
Stulting RD, Sugar A, Beck R, Belin M, Dontchev M, Feder RS, et al. Effect of donor and recipient factors on corneal graft rejection. Cornea. 2012 Oct. 31 (10):1141-7. [QxMD MEDLINE Link].
Woo JH, Ang M, Htoon HM, Tan D. Descemet Membrane Endothelial Keratoplasty Versus Descemet Stripping Automated Endothelial Keratoplasty and Penetrating Keratoplasty. Am J Ophthalmol. 2019 Nov. 207:288-303. [QxMD MEDLINE Link].
Feizi S, Javadi MA, Karimian F, Bayat K, Bineshfar N, Esfandiari H. Penetrating keratoplasty versus deep anterior lamellar keratoplasty for advanced stage of keratoconus. Am J Ophthalmol. 2022 Dec 4. [QxMD MEDLINE Link].
Alio JL, Montesel A, El Sayyad F, Barraquer RI, Arnalich-Montiel F, Alio Del Barrio JL. Corneal graft failure: an update. Br J Ophthalmol. 2021 Aug. 105 (8):1049-1058. [QxMD MEDLINE Link].
Keryn Williams, Miriam Keane, Nora Coffey, Victoria Jones, Richard Mills, Douglas Coster. The Australian Corneal Graft Registry 2018 Report. South Australian Health and Medical Research Institute. 2018. Available at https://nla.gov.au/nla.obj-726934391/view.
Sarnicola V, Toro P, Sarnicola C, Sarnicola E, Ruggiero A. Long-term graft survival in deep anterior lamellar keratoplasty. Cornea. 2012 Jun. 31 (6):621-6. [QxMD MEDLINE Link].
Yin J. Advances in corneal graft rejection. Curr Opin Ophthalmol. 2021 Jul 1. 32 (4):331-337. [QxMD MEDLINE Link].
Madi S, Leon P, Nahum Y, DʼAngelo S, Giannaccare G, Beltz J, et al. Five-Year Outcomes of Ultrathin Descemet Stripping Automated Endothelial Keratoplasty. Cornea. 2019 Sep. 38 (9):1192-1197. [QxMD MEDLINE Link].
Price MO, Price FW Jr. Descemet's membrane endothelial keratoplasty surgery: update on the evidence and hurdles to acceptance. Curr Opin Ophthalmol. 2013 Jul. 24 (4):329-35. [QxMD MEDLINE Link].
Anshu A, Price MO, Price FW Jr. Risk of corneal transplant rejection significantly reduced with Descemet's membrane endothelial keratoplasty. Ophthalmology. 2012 Mar. 119 (3):536-40. [QxMD MEDLINE Link].
Dapena I, Ham L, Netuková M, van der Wees J, Melles GR. Incidence of early allograft rejection after Descemet membrane endothelial keratoplasty. Cornea. 2011 Dec. 30 (12):1341-5. [QxMD MEDLINE Link].
Marques RE, Guerra PS, Sousa DC, Gonçalves AI, Quintas AM, Rodrigues W. DMEK versus DSAEK for Fuchs' endothelial dystrophy: A meta-analysis. Eur J Ophthalmol. 2019 Jan. 29 (1):15-22. [QxMD MEDLINE Link].
Cornea Donor Study Investigator Group, gal RL, Dontchev M, Beck RW, Mannis MJ, Holland EJ, et al. The effect of donor age on corneal transplantation outcome results of the cornea donor study. Ophthalmology. 2008 Apr. 115 (4):620-626.e6. [QxMD MEDLINE Link].
Sharma A, Sharma R. Pediatric Corneal Transplant Surgery: Challenges for Successful Outcome. Nepal J Ophthalmol. 2019 Jul. 11 (22):197-210. [QxMD MEDLINE Link].
Naacke HG, Borderie VM, Bourcier T, Touzeau O, Moldovan M, Laroche L. Outcome of Corneal transplantation rejection. Cornea. 2001 May. 20 (4):350-3. [QxMD MEDLINE Link].
Yamazoe K, Yamazoe K, Shimazaki-Den S, Shimazaki J. Prognostic factors for corneal graft recovery after severe corneal graft rejection following penetrating keratoplasty. BMC Ophthalmol. 2013 Feb 25. 13:5. [QxMD MEDLINE Link].
Panda A, Vanathi M, Kumar A, Dash Y, Priya S. Corneal graft rejection. Surv Ophthalmol. 2007 Jul-Aug. 52 (4):375-96. [QxMD MEDLINE Link].
Koay PY, Lee WH, Figueiredo FC. Opinions on risk factors and management of corneal graft rejection in the United kingdom. Cornea. 2005 Apr. 24 (3):292-6. [QxMD MEDLINE Link].
Lee HS, Kim MS. Influential factors on the survival of endothelial cells after penetrating keratoplasty. Eur J Ophthalmol. 2009 Nov-Dec. 19(6):930-5. [QxMD MEDLINE Link].
Hos D, Tuac O, Schaub F, Stanzel TP, Schrittenlocher S, Hellmich M, et al. Incidence and Clinical Course of Immune Reactions after Descemet Membrane Endothelial Keratoplasty: Retrospective Analysis of 1000 Consecutive Eyes. Ophthalmology. 2017 Apr. 124 (4):512-518. [QxMD MEDLINE Link].
Hos D, Schlereth S, Schrittenlocher S, Hayashi T, Bock F, Matthaei M, et al. [Descemet membrane endothelial keratoplasty (DMEK) for graft failure after penetrating keratoplasty and in vascularized high-risk eyes]. Ophthalmologe. 2021 Jun. 118 (6):536-543. [QxMD MEDLINE Link].
Gurnani B, Czyz CN, Mahabadi N, Havens SJ. Corneal Graft Rejection. 2022 Jan. [QxMD MEDLINE Link]. [Full Text].
Monnereau C, Bruinsma M, Ham L, Baydoun L, Oellerich S, Melles GR. Endothelial cell changes as an indicator for upcoming allograft rejection following descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2014 Sep. 158 (3):485-95. [QxMD MEDLINE Link].
Hos D, Matthaei M, Bock F, Maruyama K, Notara M, Clahsen T, et al. Immune reactions after modern lamellar (DALK, DSAEK, DMEK) versus conventional penetrating corneal transplantation. Prog Retin Eye Res. 2019 Nov. 73:100768. [QxMD MEDLINE Link].
Coster DJ, Williams KA. The impact of corneal allograft rejection on the long-term outcome of corneal transplantation. Am J Ophthalmol. 2005 Dec. 140 (6):1112-22. [QxMD MEDLINE Link].
Sel S, Schlaf G, Schurat O, Altermann WW. A novel ELISA-based crossmatch procedure to detect donor-specific anti-HLA antibodies responsible for corneal allograft rejections. J Immunol Methods. 2012 Jul 31. 381(1-2):23-31. [QxMD MEDLINE Link].
van Essen TH, Roelen DL, Williams KA, Jager MJ. Matching for Human Leukocyte Antigens (HLA) in corneal transplantation - to do or not to do. Prog Retin Eye Res. 2015 May. 46:84-110. [QxMD MEDLINE Link].
Terry MA, Aldave AJ, Szczotka-Flynn LB, Liang W, Ayala AR, Maguire MG, et al. Donor, Recipient, and Operative Factors Associated with Graft Success in the Cornea Preservation Time Study. Ophthalmology. 2018 Nov. 125 (11):1700-1709. [QxMD MEDLINE Link].
Di Zazzo A, Kheirkhah A, Abud TB, Goyal S, Dana R. Management of high-risk corneal transplantation. Surv Ophthalmol. 2017 Nov-Dec. 62 (6):816-827. [QxMD MEDLINE Link].
Baydoun L, Bruinsma M, Santander-García D, Ham L, Oellerich S, Melles GRJ. Combined specular microscopy and Scheimpflug imaging to improve detection of an upcoming allograft rejection after DMEK. Acta Ophthalmol. 2020 May. 98 (3):261-266. [QxMD MEDLINE Link].
Chirapapaisan C, Abbouda A, Jamali A, Müller RT, Cavalcanti BM, Colon C, et al. In Vivo Confocal Microscopy Demonstrates Increased Immune Cell Densities in Corneal Graft Rejection Correlating With Signs and Symptoms. Am J Ophthalmol. 2019 Jul. 203:26-36. [QxMD MEDLINE Link].
Smith C, Kaitis D, Winegar J, Edelstein S, Council M, Kontadakis G, et al. Comparison of endothelial/Descemet's membrane complex thickness with endothelial cell density for the diagnosis of corneal transplant rejection. Ther Adv Ophthalmol. 2018 Jan-Dec. 10:2515841418814187. [QxMD MEDLINE Link].
Shahrudin NA, Mohd Zahidin AZ, Md Noh UK, Wan Abdul Halim WH, Md Din N. CMV endotheliitis: a cause for recurrent failed corneal transplant. GMS Ophthalmol Cases. 2017. 7:Doc31. [QxMD MEDLINE Link].
Shahrudin NA, Mohd Zahidin AZ, Md Noh UK, Wan Abdul Halim WH, Md Din N. CMV endotheliitis: a cause for recurrent failed corneal transplant. GMS Ophthalmol Cases. 2017. 7:Doc31. [QxMD MEDLINE Link].
Hill JC, Maske R, Watson P. Corticosteroids in corneal graft rejection. Oral versus single pulse therapy. Ophthalmology. 1991 Mar. 98 (3):329-33. [QxMD MEDLINE Link].
Birnbaum F, Böhringer D, Sokolovska Y, Sundmacher R, Reinhard T. Immunosuppression with cyclosporine A and mycophenolate mofetil after penetrating high-risk keratoplasty: a retrospective study. Transplantation. 2005 Apr 27. 79 (8):964-8. [QxMD MEDLINE Link].
Chatel MA, Larkin DF. Sirolimus and mycophenolate as combination prophylaxis in corneal transplant recipients at high rejection risk. Am J Ophthalmol. 2010 Aug. 150 (2):179-84. [QxMD MEDLINE Link].
Zhai LY, Zhang XR, Liu H, Ma Y, Xu HC. Observation of topical tacrolimus on high-risk penetrating keratoplasty patients: a randomized clinical trial study. Eye (Lond). 2020 Sep. 34 (9):1600-1607. [QxMD MEDLINE Link].
Szaflik JP, Major J, Izdebska J, Lao M, Szaflik J. Systemic immunosuppression with mycophenolate mofetil to prevent corneal graft rejection after high-risk penetrating keratoplasty: a 2-year follow-up study. Graefes Arch Clin Exp Ophthalmol. 2016 Feb. 254 (2):307-14. [QxMD MEDLINE Link].
Birnbaum F, Mayweg S, Reis A, Böhringer D, Seitz B, Engelmann K, et al. Mycophenolate mofetil (MMF) following penetrating high-risk keratoplasty: long-term results of a prospective, randomised, multicentre study. Eye (Lond). 2009 Nov. 23 (11):2063-70. [QxMD MEDLINE Link].
Schmitz K, Hitzer S, Behrens-Baumann W. [Immune suppression by combination therapy with basiliximab and cyclosporin in high risk keratoplasty. A pilot study]. Ophthalmologe. 2002 Jan. 99 (1):38-45. [QxMD MEDLINE Link].
Stanojlovic S, Schlickeiser S, Appelt C, Vogt K, Schmitt-Knosalla I, Haase S, et al. Influence of combined treatment of low dose rapamycin and cyclosporin A on corneal allograft survival. Graefes Arch Clin Exp Ophthalmol. 2010 Oct. 248 (10):1447-56. [QxMD MEDLINE Link].
Nguyen P, Barte F, Shinada S, Yiu SC. Management of Corneal Graft Rejection - A Case Series Report and Review of the Literature. J Clin Exp Ophthalmol. 2010 Sep 29. 1 (103):[QxMD MEDLINE Link].
Gebhardt BM, Varnell ED, Kaufman HE. Cyclosporine in collagen particles: corneal penetration and suppression of allograft rejection. J Ocul Pharmacol Ther. 1995 Winter. 11 (4):509-17. [QxMD MEDLINE Link].
Azevedo Magalhaes O, Shalaby Bardan A, Zarei-Ghanavati M, Liu C. Literature review and suggested protocol for prevention and treatment of corneal graft rejection. Eye (Lond). 2020 Mar. 34 (3):442-450. [QxMD MEDLINE Link].
Kuo HH, Shen EP. Long-term topical bevacizumab for prevention of corneal graft rejections. Eur J Ophthalmol. 2021 Nov. 31 (6):NP48-NP52. [QxMD MEDLINE Link].
Hos D, Le VNH, Hellmich M, Siebelmann S, Roters S, Bachmann BO, et al. Risk of Corneal Graft Rejection After High-risk Keratoplasty Following Fine-needle Vessel Coagulation of Corneal Neovascularization Combined With Bevacizumab: A Pilot Study. Transplant Direct. 2019 May. 5 (5):e452. [QxMD MEDLINE Link].
Schaub F, Hou Y, Zhang W, Bock F, Hos D, Cursiefen C. Corneal Crosslinking to Regress Pathologic Corneal Neovascularization Before High-Risk Keratoplasty. Cornea. 2021 Feb 1. 40 (2):147-155. [QxMD MEDLINE Link].
Kumar A, Yun H, Funderburgh ML, Du Y. Regenerative therapy for the Cornea. Prog Retin Eye Res. 2022 Mar. 87:101011. [QxMD MEDLINE Link].
Qin Q, Shi Y, Zhao Q, Luo D, Chen Y, Wu J, et al. Effects of CD25siRNA gene transfer on high-risk rat corneal graft rejection. Graefes Arch Clin Exp Ophthalmol. 2015 Oct. 253 (10):1765-76. [QxMD MEDLINE Link].
Yoon CH, Choi HJ, Kim MK. Corneal xenotransplantation: Where are we standing?. Prog Retin Eye Res. 2021 Jan. 80:100876. [QxMD MEDLINE Link].
Ritter T, Wilk M, Nosov M. Gene therapy approaches to prevent corneal graft rejection: where do we stand?. Ophthalmic Res. 2013. 50(3):135-40. [QxMD MEDLINE Link].
Panda A, Vanathi M, Kumar A, Dash Y, Priya S. Corneal graft rejection. Surv Ophthalmol. 2007 Jul-Aug. 52 (4):375-96. [QxMD MEDLINE Link].
Ang M, Wilkins MR, Mehta JS, Tan D. Descemet membrane endothelial keratoplasty. Br J Ophthalmol. 2016 Jan. 100 (1):15-21. [QxMD MEDLINE Link].
Guerra FP, Anshu A, Price MO, Giebel AW, Price FW. Descemet's membrane endothelial keratoplasty: prospective study of 1-year visual outcomes, graft survival, and endothelial cell loss. Ophthalmology. 2011 Dec. 118 (12):2368-73. [QxMD MEDLINE Link].
Keenan TD, Jones MN, Rushton S, Carley FM. Trends in the indications for corneal graft surgery in the United Kingdom: 1999 through 2009. Arch Ophthalmol. 2012 May 1. 130(5):621-8. [QxMD MEDLINE Link].
Boisjoly HM, Tourigny R, Bazin R, Laughrea PA, Dube I, Chamberland G, et al. Risk factors of corneal graft failure. Ophthalmology. 1993 Nov. 100(11):1728-35. [QxMD MEDLINE Link].
Chen YF, Gebhardt BM, Reidy JJ, Kaufman HE. Cyclosporine-containing collagen shields suppress corneal allograft rejection. Am J Ophthalmol. 1990 Feb 15. 109(2):132-7. [QxMD MEDLINE Link].
Hegde S, Beauregard C, Mayhew E. CD4(+) T-cell-mediated mechanisms of corneal allograft rejection: role of Fas-induced apoptosis. Transplantation. 2005 Jan 15. 79(1):23-31. [QxMD MEDLINE Link].
Hill JC. Systemic cyclosporine in high-risk keratoplasty. Short- versus long-term therapy. Ophthalmology. 1994 Jan. 101(1):128-33. [QxMD MEDLINE Link].
Hill JC. The use of cyclosporine in high-risk keratoplasty. Am J Ophthalmol. 1989 May 15. 107(5):506-10. [QxMD MEDLINE Link].
Hill JC, Maske R, Watson P. Corticosteroids in corneal graft rejection. Oral versus single pulse therapy. Ophthalmology. 1991 Mar. 98(3):329-33. [QxMD MEDLINE Link].
Hwang DG, Stern WH, Hwang PH, MacGowan-Smith LA. Collagen shield enhancement of topical dexamethasone penetration. Arch Ophthalmol. 1989 Sep. 107(9):1375-80. [QxMD MEDLINE Link].
Khodadoust AA, Silverstein AM. Transplantation and rejection of individual layers of the cornea. Investigative Ophthalmologic and Visual Sciences. Vol 8.: 180-195.
Reidy JJ, Gebhardt BM, Kaufman HE. The collagen shield. A new vehicle for delivery of cyclosporin A to the eye. Cornea. 1990 Jul. 9(3):196-9. [QxMD MEDLINE Link].
Smolin G, Thoft RA. The cornea. Scientific Foundations and Clinical Practice. 3rd ed. Lippincott William & Wilkins; 1994.
Wang M, Lin Y, Chen J, Liu Y, Xie H, Ye C. Studies on the effects of the immunosuppressant FK-506 on the high-risk corneal graft rejection. Yan Ke Xue Bao. 2002 Sep. 18(3):160-4. [QxMD MEDLINE Link].
Wilson SE, Kaufman HE. Graft failure after penetrating keratoplasty. Surv Ophthalmol. 1990 Mar-Apr. 34(5):325-56. [QxMD MEDLINE Link].
 This severely vascularized cornea would be at high risk for graft rejection following a penetrating keratoplasty. This patient experienced Stevens-Johnson syndrome.
This severely vascularized cornea would be at high risk for graft rejection following a penetrating keratoplasty. This patient experienced Stevens-Johnson syndrome.
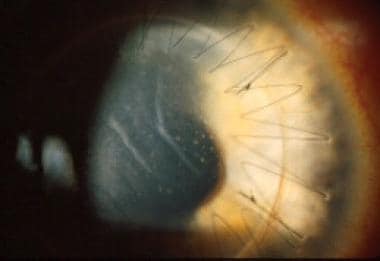 This is an example of an acute graft rejection episode. Note the graft edema, Descemet folds, and keratic precipitates.
This is an example of an acute graft rejection episode. Note the graft edema, Descemet folds, and keratic precipitates.

