Common Skin Infections
| Site: | QMplus - The Online Learning Environment of Queen Mary University of London |
| Module: | PG DipClinDerm Sample Course |
| Book: | Common Skin Infections |
| Printed by: | Guest user |
| Date: | Tuesday, 16 April 2024, 10:51 AM |
Description
Common skin infections
Table of contents
- Objectives
- Common Skin Infections
- Introduction
- Bacterial Infections
- Impetigo and Cellulitis
- Folliculitis and Boils
- Hidradenitis Suppurativa and Echthyma
- 'Often Missed' Streptococcal Diagnoses
- SSSS and Toxic Shock Syndrome
- PVL and MRSA, Strep Toxic Shock Syndrome
- Scarlet Fever and Meningococcal Disease
- Invasive Infections
- Infections Caused by Corynebacterium and Pitted Keratolysis
- VIRAL INFECTIONS
- Varicella Zoster and Herpes Zoster
- Primary Herpes Simplex Infection
- Other Viral Causes of Vesicular Rashes
- Parvovirus Infection 'Slapped Check'
- Rubella
- Measles and Roseola infantum
- Other Main Causative Agents of a Maculopapular Rash
- Warts
- Molluscum Contagiosum
- FUNGAL DISEASES
- Diseases Caused by Moulds
- Common Parasitic Infections
- Key Learning Points
- Supplementary Material
- Multimedia Resources
MODULE 1 – Week 3
Introduction and Common Dermatological Problems - Common Skin Infections
Objectives
At the end of this module course participants should be able to:
- List the bacteria commonly involved in skin infection
- Recognise the clinical features of common bacterial infections, including impetigo, cellulites, folliculitis, boils
- Recognise rarer bacterial infections such as staphylococcal scalded skin syndrome, toxic shock syndrome, necrotising fasciitis
- Describe how to investigate a patient with suspected bacterial infection
- Formulate a management plan for a patient with a bacterial infection
- List the main viruses involved in skin disease
- Recognise the clinical features of common viral infections, including herpes simplex, varicella zoster, measles, rubella, viral warts, molluscum contagiosum
- Be able to counsel a pregnant woman who has had contact with chickenpox, rubella
- Describe the specific problems that viruses may cause in patients with eczema or the immunocompromised
- Discuss the treatment available for viral infections
- Recognise fungal infections of the skin including tinea
- Differentiate between fungal and yeast infections of the skin
- Be able to do a fungal skin scraping
- Discuss treatments available for fungal infection
Click here to return
MODULE 1 – Week 3
Introduction and Common Dermatological Problems - Common Skin Infections
Common Skin Infections
This week we will be looking at some of the more common pathogens which affect the skin in European countries. Mycobacterial disease, cutaneous manifestations of HIV disease, parasitic infestations and tropical diseases are covered in Module 5.
BACTERIAL INFECTIONS
Thanks to the introduction of antibiotics and improvements to sanitation and living conditions, bacterial infections are much less of a problem in many parts of the world than, say, 30 years ago. Nonetheless, increasing antibiotic resistance and emergence of virulent strains such as Panton- Valentin Leucocidin Staphylococci mean that these are shifting sands, and recognition and swift treatment of cutaneous bacterial infections remains as important now as then.
There are 3 key features to the development of bacterial infection:
- The integrity of the epidermis - provides a barrier to entry by bacteria. This is one reason why patients with altered barrier function in atopic eczema (and with filaggrin mutations) have such problems with staphylococcal super-colonisation and infection.
- The skin's normal bacterial (and fungal) flora prevent colonisation by pathogenic organisms.
- Host immunity.
Infection normally requires a small break in epidermal integrity to gain access such as trauma, leg ulcers, surgical wounds, IV drug user injection sites, fungal infections (e.g. athlete's foot). Also, abnormal scaling of the skin (e.g. in eczema) encourages bacterial adherence. Immunosuppression (Diabetes Mellitus, AIDS, drugs) is associated with an increased incidence of infection.
- In the UK, Impetigo/cellulitis/boils (usually staphylococcal driven) are the most common infections we see, whereas in developing countries TB, Leprosy and impetigo account for most cutaneous infections.
STREPTOCOCCAL AND STAPHYLOCOCCAL INFECTIONS
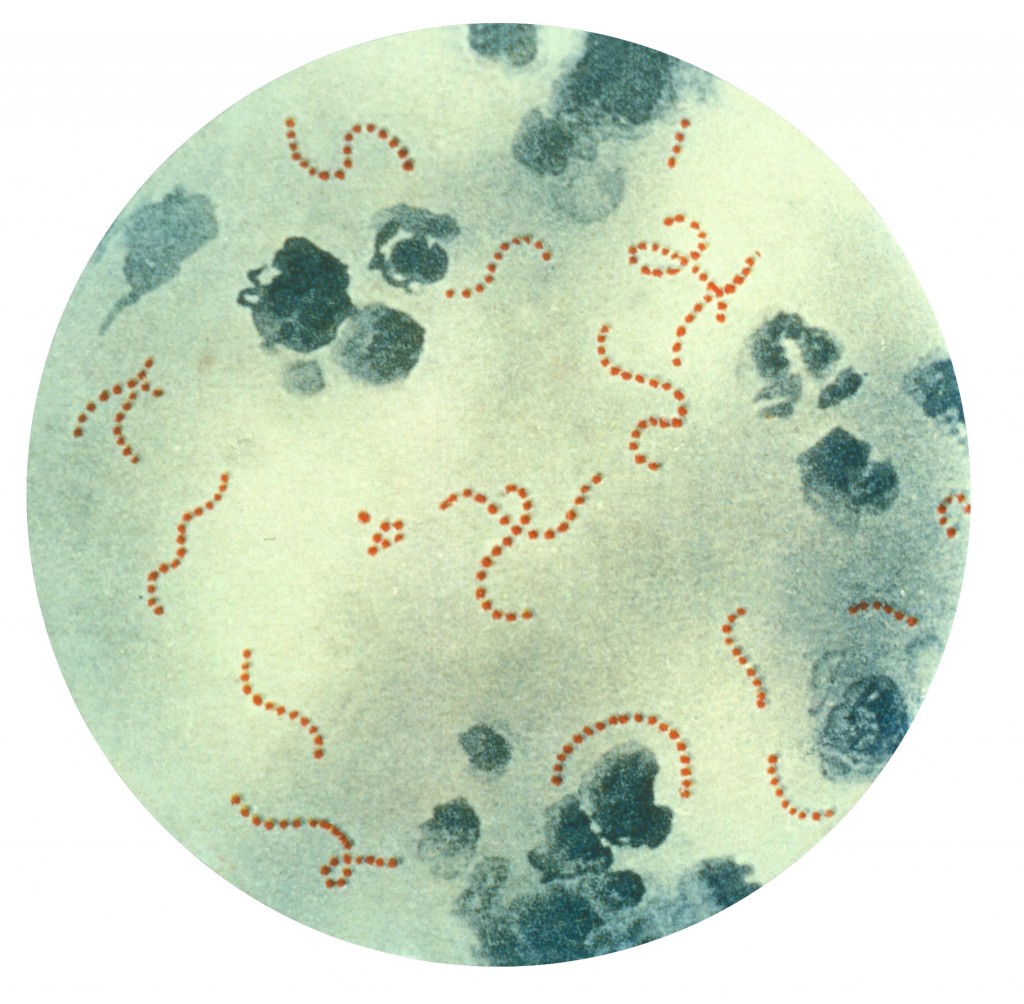
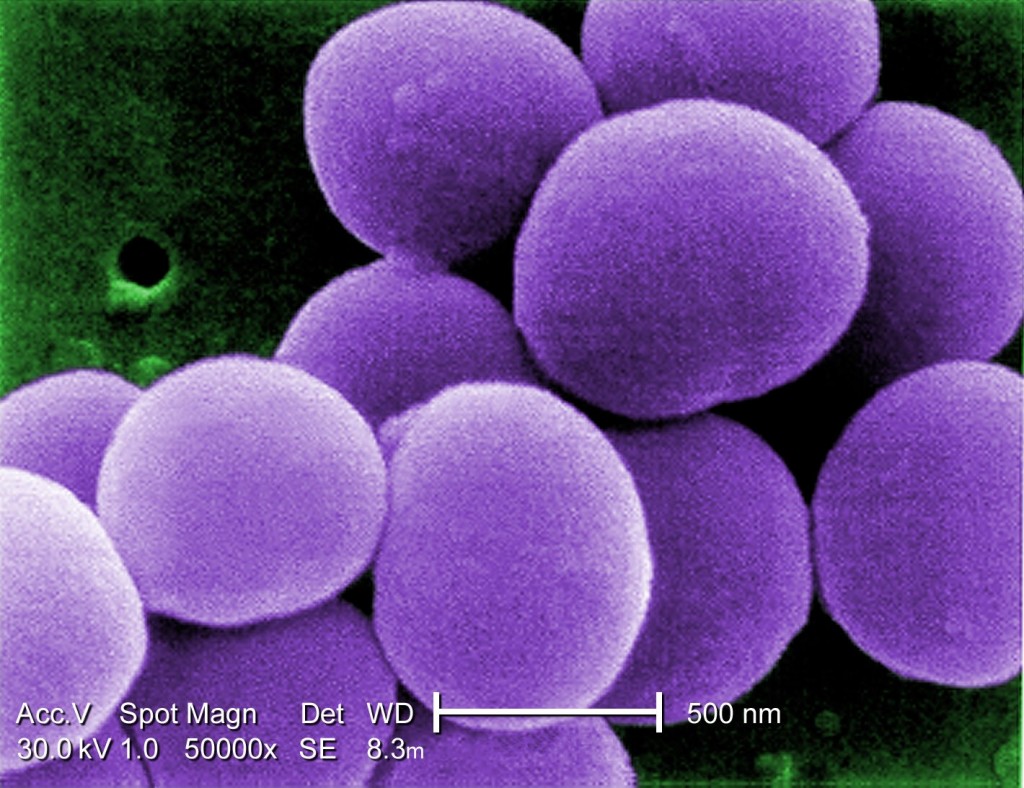
Streptococcus sp Staphylococcus aureus
Impetigo
Unlike most skin disease, impetigo is a highly infectious skin disease (spread by direct contact - family/school). It is a very common condition and is most common in children. It typically presents with weeping, exudative areas with a typical honey coloured crust on the surface (esp face and hands). If you see it in an adult, you should consider whether the patient plays contact sports ('scrum pox' when spread by rugby players), has an underlying immune disorder, or whether you are seeing 'impetiginisation' of another dermatological problem i.e. secondary staphylococcal infection superimposed on a primary dermatological condition such as nummular dermatitis. It can cause blistering ("bullous impetigo") due to bacterial toxins. Over 90% of cases are caused by Staphylococcus aureus, but rarely group A Streptococci can be responsible, so taking swabs is important.


Bullous impetigo in a child. Note annular appearance Impetigo in an adult (HIV associated)
We probably overuse oral antibiotics for this condition. Localised disease can be treated with topical fucidin (three times daily) and the antiseptic povidone iodine for 1 week. In very weepy impetiginised eczema I sometimes suggest using Potassium permanganate soaks (dilute KMNO4 to pale pink solution and apply on gauze for 20 mins. Remember it stains nails and washbasins etc brown - make it up as a dilution on an old plastic bowl not the posh sink!). For more extensive disease, oral antibiotics for 7-10 days (flucloxacillin 500mg four times daily for staphylococcus; Penicillin V 500mg four times daily for streptococcus) should be used. In hospital practice we often use a combination such as CoAmoxiclav but in the community setting this practice has recently been discouraged due to the threat of increased bacterial resistance. Other close contacts should be examined and children should avoid school whilst lesions are weepy and crusty. Recurrent impetigo may occur, often due to resistant bacteria e.g. MRSA. In these cases take skin swabs for bacteria (MRSA) and check other family members. I often take nasal swabs and consider Nasal staphylococcal eradication – e.g. mupirocin (three times daily for 1 week) to eradicate nasal carriage +/-treat whole family with antibiotics/chlorhexidine. If this doesn't work, then you should consider whether there is underlying immunosuppression/diabetes.
Cellulitis
Cellulitis is a hot, sometimes tender area of confluent erythema of the skin and is usually caused by a streptococcus (occasionally staph/gram negatives). There may be a portal of entry for infection such as a recent abrasion or a venous leg ulcer. Web spaces of the toes should be examined for evidence of fungal infection. It often affects the lower leg causing an upwards spreading, hot erythema. Patients are nearly always unwell and pyrexial. It may also be seen affecting one side of the face - hot, well-demarcated swollen erythema- when it is known as Erysipelas.
Clinical Tip; Erysipelas often starts just under the eye or at the bridge of the nose and has a surprising amount of oedema. It may resemble an allergic contact dermatitis initially but the clue is that in erysipelas the patient is unwell.
Occasionally, as well as the signs described above, one can see blistering of the skin.
Diagnosis is nearly always made on clinical grounds as blood cultures are often negative. Confirmation of infection, if necessary, is best done serologically by streptococcal titres (ASOT).
In the early stages oral Penicillin or Erythromycin 500 mg twice daily (bd) may suffice. However it is important to have a low threshold for admission to hospital for IV antibiotics as cellulitis may be fatal. It may be recurrent, particularly in those patients with underlying lymphoedema or venous hypertension, and long term low dose antibiotic prophylaxis should be considered in high risk individuals.
Clinical Tip: Note that cellulitis is unilateral! It is VERY rare to see it bilaterally. Junior casualty officers often refer 'bilateral cellulitis' when in fact the diagnosis is usually varicose eczema with venous hypertension, allergic contact dermatitis to bandages or lipodermatosclerosis.
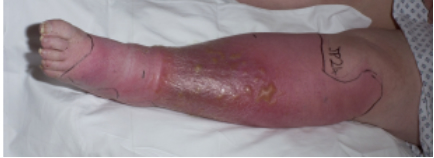
Cellulitis – hot, red leg. Note blistering also.

Post-operative cellulitis – note the marking to indicate if improvement occurring

Erysipelas of ear

Erysipelas- note the typical initial location under eye and at bridge of nose with significant oedema
Dissecting Cellulitis of the Scalp is really rather a misnomer as it is not a cellulitis! it is a condition seen young to middle-aged men with skin type 6 and consists of painless, deep, firm nodules, over the scalp. There may be marked bogginess and sinus tracts. Treatment is difficult but oral tetracyclines or intralesional corticosteroids. It is discussed in more detail in the module on Hair Disorders. I include it here for completeness.
Folliculitis and Boils
Folliculitis, by definition, is an inflammation centered around and of the hair follicle. Clinically one sees folliculocentric itchy or tender papulopustules, often with a central hair protruding from them. Superficial infection - usually staphylococcus aureus - produces the clinical appearance of folliculitis, whereas more deep seated infection results in boils or carbuncles (large boils).

Folliculitis - note visible hair emerging from folliculocentric pustule

Pseudofolliculitis is the term used for a folliculitis due to ingrowing hairs rather than true primary bacterial infection (e.g. shaving rash of beard area or shaved/waxed legs). The main problem here is inflammation due to the irritation of the hairs rather than primary bacterial infection. However the two conditions overlap in practice. "Sycosis barbae" is yet another term - implying an infected shaving rash but again hair irritation plays a role as well. Advising the patient to leave a small length of beard and to use clippers rather than an electric razor may help. I sometime suggest topical anti fungal/weak steroid combination once week after shaving to help keep it at bay.

Sycosis barbae-commoner in skin type 6
There are lots of causes of folliculitls and indeed the cause may be multifactorial - infection, shaving practices, racial (genetic) variation, climate/humidity, occlusive clothes, occlusive medical dressings, use of very greasy moisturisers, rich ointments or hair pomades.
There are a number of specific 'folliculitis' entities which are worth knowing about - some more common than others.
1. Hot-tub folliculitis -Unhygienic jacuzzis can be a source of infection which is due to pseudomonas. This often spontaneously resolves but can be treated with topical antibiotic if needed.

'Hot-tub'pseudomonas folliculitis. Note cut off at waist with lesions only in immersed areas.
2. Pityrosporum folliculitis on trunk (see below in ' fungal' section). Note very monomorphic lesions.

Pityrosporum folliculits. Often seen in athletes or those who work in hot, sweaty environments
3. "Steroid acne" is a folliculitis secondary to systemic steroids (it is not a true acne but rather is an acneiform eruption).

Steroid acne- associated with use of oral steroids. Note how monomorphic the lesions are in this typical location for this diagnosis.
4. "Itchy folliculitis" is a very itchy folliculocentric eruption seen on the upper trunk and limbs, secondary to HIV infection (cause unknown). It has many eosinophils histologically and usually responds to Tetracyclines, but it is important to know about it as it can be a presenting sign of HIV infection. It has sometimes been called 'eosinophilic folliculitis'.

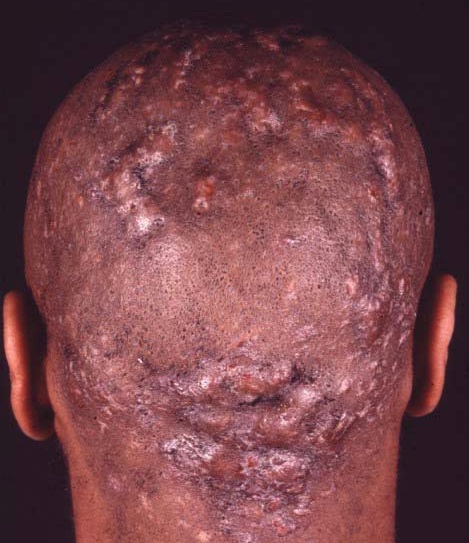
5. Folliculitis (or acne) keloidalis – This is very common in young black adult males. It is a 'folliculitis' on the nape of neck and occipital scalp which can progress to hypertrophic scars or keloid with hair loss. Occasionally the condition is very severe with deeper infection – the whole occipital scalp is boggy and discharging with scarring alopecia (called "dissecting cellulitis of scalp" or "perifolliculitis capitis") Treatment is very difficult. Try avoiding shaving and long-term (more than 6 months) oral antibiotics. For severe cases triamcinolone injection into the scarred area or radical surgery is indicated. It is not really a true folliculitis in the bacterial sense but is included here for completeness.

Treatment of folliculitis: "Infective form" is with topical antiseptics, topical antibiotics (e.g. fusidic acid) or oral antibiotics (e.g. flucloxacillin 500mg or erythromycin 500mg both four times daily for 2-4 weeks or longer). Remember to think about itchy folliculitis in widespread chest folliculitis and whether any element of occlusion with grease or ointments is provoking the problem. Advise patients to avoid tight clothes, occlusive dressings, use lighter moisturisers, and to rub moisturisers in the direction of hair growth etc. "In-growing hair form" - avoid shaving if possible or shave less closely, without stretching the skin. I often use a weak hydrocortisone-fungal combination after shaving as a precautionary measure and many patients find this helpful.
Hidradenitis suppurativa
I have included this condition under BOILS, although it is not a true staphylococcal/streptococcal infectious boil as such, but rather an inflammatory one which may be part of the so-called Follicular Occlusion Tetrad of conditions- Hidradenitis, Dissecting Cellulitis, Acne Conglobata and Pilonidal sinus. I have put it here though as patients usually present with what they describe as 'recurrent boils', and it is an important condition to be aware of. Fortunately it is a relatively rare condition but one which causes a vast amount of suffering to the patient. It is characterised by a painful, discharging, chronic inflammation of the skin at sites rich in apocrine glands (axillae, groins, natal cleft). Patients tend to be females usually, but not always, with a high BMI and within some families it appears to be inherited in an autosomal dominant fashion. It presents after puberty with paired comedones, papules, nodules and abscesses which often progress to cysts and sinus formation. Lesions are in the axillae, groin, natal cleft and buttocks. Complications include fistulae, keloid scars, lymphoedema and contractures. The condition follows a chronic relapsing remitting course and aggravated by obesity, smoking and certain drugs e.g. Lithium. It is thought to be multifactorial - hormones, infection, apocrine gland structure and genetic predisposition (PSENEN & NCSTN genes). Treatment is very difficult, particularly in moderate and severe disease and involves lifestyle measures such as stop smoking, lose weight, topical antispetics e.g. Chlorhexidine as soap. Mild disease can be managed with topical antibiotics such as Erythromycin and Clindamycin, along with staph elimination and bleach baths.
There are a number of therapeutic options for more severe disease which can often be very difficult to control, and include oral antibiotics: Tetracyclines, Clindamycin +/- Rifampicin, oral antiandrogens, isotretinoin/acitretin and in very severe cases biologic therapy with Infliximab. Surgery may be indicated. There is some suggestion that oral zinc sulphate 10mg/kg max 400-600 mg daily may be helpful in Hidradenitis, and a number of case reports using axillary Botox have suggested that this may be of benefit also.

Hidradenitis- typical locations and note typical bridging scarring in axilla.
Echthyma
This is an infection due to streptococcus or staphylococcus aureus or occasionally both which is rare in the UK but seen more commonly in debilitated, intravenous drug abusers immunosuppressed people (e.g. HIV), diabetics, the homeless alcoholics etc. It is more common in developing countries, being associated with poor nutrition and hygiene. Typically, chronic well demarcated, round, ulcerative lesions sometimes with an exudative crust are seen usually on the lower legs. Eschar like appearances can be noted and associated ulceration can be deep. It can usually be treated with oral antibiotics but remember if you do encounter a case to look for an underlying cause.

Echthyma – note the deep, black, crusted ulcers
3 'Often missed ' stretococcal diagnoses
Perianal streptococcal cellulitis - quite common in children under age 10. Presents with perianal redness and soreness that may make defaecation painful. No systemic upset. Check skin swab for Streptococcus pyogenes. Responds to oral penicillin.

Streptococcal vulvo-vaginitis – usually caused by Strep. pyogenes presents as vulvo-vaginitis in pre-pubertal girls. Presents with genital soreness, dysuria and sometimes purulent discharge. Treatment - oral penicillin. Both the above can rarely occur in adults.

Blistering distal dactylitis A large blister/pustule on tip of a finger (palmar) esp in children/young adults - swab it - responds to oral penicillin.

Toxin mediated Staphylococcal and Streptococcal diseases.
The conditions which we have just seen and discussed are all due to direct invasion of the tissue by the bacterium. Both staphylococci and streptococci can cause pathology by toxins and we will have a look at these here. Although this is not discussed further at this stage in the course, remember too that Streptococcal throat infection may cause exacerbation of psoriasis by antigen cross linkage in the skin.
Staphylococcal Scalded Skin Syndrome (SSSS)
Staphylococcal scalded skin syndrome (SSSS) is the most common of the toxin mediated disorders but even so, is fortunately rare. It presents as an acute toxic illness in children and is exceptionally rare in adults. The skin becomes bright red with superficial blisters and shedding (like a scald).
Clinical Tip - often starting in flexures and body folds with peeling skin.
Systemic upset with fever is usual and unlike toxic epidermal necrolysis (which it can mimic) there is no mucosal involvement. Staph aureus produces a toxin which attacks the outer part of epidermis, causing the typical peeling.

Staphylococcal scalded skin syndrome – unwell child, with red, peeling skin, initially flexural involvement
Prognosis is very good if treated with antibiotics (flucloxacillin). Remember that only the outer epidermis is damaged. The inner epidermis is preserved which preserves most of skin function (unlike in Toxic epidermal necrolysis where one sees full thickness epidermal necrosis). Patients should be seen by a dermatologist as an emergency.
Toxic shock syndrome
This is best known for occurring in tampon users. It is luckily fairly rare but can be fatal. Fever and an initial faint macular erythema or scarlatiniform rash is typical in the beginning, with mucosal erythema a common sign. 1-3 weeks later circulatory shock and multi-system disease occurs. Treatment involves antibiotics and supportive care.
Clinical Tip: Shocked female patients -ask if they are menstruating and using tampons.
Panton-Valentine leukocidin (PVL) associated disease and MRSA
PVL is a pore-forming toxin produced by several strains of staph aureus including community - acquired methicillin-resistant staph aureus. It is associated with recurrent and necrotic skin and soft-tissue infections. Risk factors include compromised skin integrity; skin-to-skin contact with infected individuals and sharing of contaminated towels. It is common in students sharing accommodation and in individuals such as wrestlers or those indulging in contact sports. I recently saw a case of beard furunculosis due to PVL staphs in a professional cage-fighter. Infection of the hair follicle is the most common PVL-associated disease and usually presents as a large skin abscess, boils or furuncles with surrounding erythema. The lesions are often multiple and are often associated with systemic upset, e.g. fever. You need to specifically request PVL testing on the swab if you are suspicious of PVL, as labs won't routinely do it.
The treatment of choice is surgical drainage of the abscess but if antibiotics are needed, Clindamycin, Linezolid and Rifampicin can be used although specialist microbiology advice should be sought in these cases.
Clinical Tip: Occurs in students, contact sports, deep abscesses
One of the reasons why PVL staphs are important to recognise is that it can cause widespread septicaemia and pulmonary infection and fatalities have been reported.
Clinical Tip: Get patients to stop smoking if they have had MRSA/PVL infections
Clinical Tip: MRSA /PVL patients and their families should be advised to decolonise their living environments by using alcohol wipes/gel to toilet handles/computer keyboards/fridge doors etc and decontaminate pets

PVL staph abscesses in a teenage patient
Streptococcal toxic shock syndrome is very similar to the above, associated with invasive Group A Strep (throat, wounds, soft-tissue).
Scarlet fever is caused by Strep pyogenes (a Group A strep) usually from a sore-throat, which produces a toxin. There is fever, then 1-2 days later, punctate erythema progressing to erythroderma (mild purpura in skin creases and perioral sparing is characteristic). Mucosal erythema is common. By day 7-10 skin shedding occurs. It can occasionally be very severe and coma and myocarditits have been reported. Complications also include suppurative: arthritis, meningitis, and osteomyelitis. Fortunately it is much less common than in the last century and also less severe. Treatment - penicillin and supportive care.

Scarlet fever
Meningococcal disease
Although this is not a skin disease as such, the presence of purpura on the skin is such an important clinical sign not to be missed that I feel duty bound to include it in this chapter. Remember your patient may be feverish, have a headache and photophobia but they may not look unduly unwell at the beginning so LOOK AT THE SKIN very carefully all over.
Clinical Tip: Meningococcal purpura, unlike a leucocytoclastic vasculitis which tend to favour the lower legs, can occur anywhere on the body, with non blanching often irregularly shaped purpuric or dusky skin changes.

Meningococcal sepsis- note non blanching irregularly shaped purpura
Invasive Infections
Thank goodness these are rare but I have included them here as they are very often fatal and again it is imperative not to miss them.
- Necrotising fasciitis This occurs most commonly in elderly, debilitated and diabetic especially post-surgery. It may be streptococcal or due to mixed infection. The patient may not be toxic in the early stages but the most striking finding is of severe pain, often seeming to be out of proportion to what one sees on the skin surface. Tender erythematous skin evolves into a rapidly spreading area of black necrosis around the wound. Treatment is with immediate extensive surgical debridement, antibiotics and supportive care.

- "Fournier's gangrene" is a version of the above that often starts in the scrotum/lower abdomen.

Infections caused by Corynebacterium
Corynebacterium (the bug also responsible for Diphtheria) can cause 3 rashes:
Erythrasma
Presents as an orangy-brown flexural rash often seen in the axillae or toe web spaces. It is frequently misdiagnosed as a fungal infection but the very distinct colour is usually helpful in making the diagnosis. The rash shows a dramatic coral pink fluorescence under Wood's (ultraviolet) light. It is caused by Corynebacterium minutissimum and is easily treated with Erythromycin either orally or I often use the topical form which is licensed for use in acne. -oral Erythromycin (500mg four times daily for 10 days).
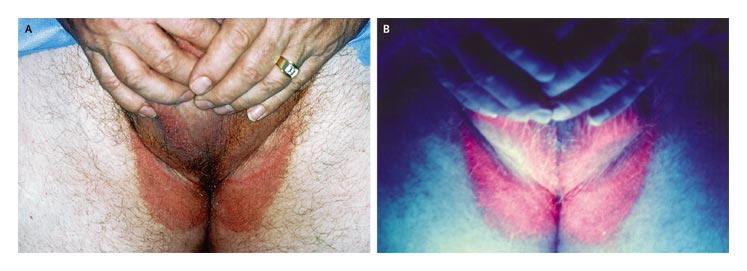
Erythrasma – orangy-brown rash in groin Fluoresces pink under Wood’s light
Pitted keratolysis
This is a superficial infection of the horny layer of the skin frequently involves the soles of the forefoot and appears as numerous small punched-out circular lesions of a rather macerated skin (e.g. as seen after prolonged immersion). There is usually an associated hyperhidrosis of the feet and a prominent odour. It can be confused with mosaic warts but when you look carefully you will see that there are pits rather than black dots (which are seen in warts).
Treatment: topical antibiotics (e.g. fusidic acid, clindamycin or erythromycin; apply twice daily for 2-4 weeks) and topical anti-sweating lotions.

Pitted keratolysis - clustered white punched-out pits
VIRAL INFECTIONS
Viruses can cause many different appearances on the skin! Rashes or lesions caused by viruses may be -
- Macular
- Maculopapular
- Vesicular
- Purpuric
- Warty
1. Vesicular rashes
Typically rashes with vesicles tend to be caused by one of the following.
- Herpes simplex
- Varicella zoster
- Poxviruses
- Coxsackie virus
- Entero/echo viruses
Herpes zoster and varicella zoster
Varicella is the term used to describe classical ‘chickenpox’. The incubation period is 21 days and there may be an influenza – like prodrome prior to the rash. The rash classically starts centrally and then spreads, particularly to areas not exposed to pressure e.g. axillae; it is rare on the palms or soles. Lesions appear in crops, initially appearing as macules and then developing into papules, which become vesicular and then crust as the vesicles burst. There are usually lesions at all stages visible. Recovery from infection gives lifelong immunity. The virus remains latent in one or more posterior root ganglia. Remember infection may be more severe in adults, in immunocompromised and in smokers who are at risk of developing Chicken pox pneumonitis.
Clinical Tip: Look in Axillae (often involved) and look for lesion 'Dew Drop on a Rose Petal'- vesicle on erythematous base

Varicella – note lesions at different stages in development

Dew Drop on Rose Petal
Herpes zoster refers to the reactivation of varicella zoster virus causing a unilateral rash in a single dermatome (shingles), most commonly the ophthalmic branch of the trigeminal nerve and on the trunk in the distribution of T5-L2. The rash may be preceded by an area of paraesthesia and hyperaesthesia where the rash develops and with weakness in the affected or adjoining limb. The rash is also vesicular and heals with crusting. The majority of cases occur over the age of 50 years.
Clinical Tip: Asking about preceeding dysaesthesia in the skin is a really helpful way to aid making the diagnosis, particularly if you are not sure.

Herpes zoster – note the dermatomal distribution
What if the rash is not confined to one dermatome? How can you determine whether the infection is primary or a reactivation (shingles)?
This is initially determined from the history. Questions to ask:
- Is there a history of chickenpox
- Has there been any contact with chickenpox? Patients are infectious from 24-48 hours prior to the rash and until all vesicles have crusted, usually 5-7 days. Spread occurs via respiratory droplets. In practice spread will only occur after a prolonged period of time in close proximity e.g. 15 mins face to face contact or 30 mins in the same room. Contact prior to 48 hours before the rash can be disregarded.
- What age is the patient? Zoster is more common in the elderly, but may occur in children with a history of varicella occurring in utero or in infancy. Healthy children presenting with shingles therefore may sometimes need to be investigated for causes of immunosuppression.
- Is the patient immunosuppressed? Very immunosuppressed patients e.g. those receiving chemotherapy, may occasionally present with ‘disseminated shingles’ i.e. several dermatomes affected. They will also be generally unwell with a fever and tachycardia and should be referred to hospital for intravenous Aciclovir.
Clinical Tip: Multi-dermatomal shingles can be a presenting sign of HIV infection and should ring alarm bells.
Laboratory diagnosis
1 Serology: is this primary or secondary? If it is unclear whether the patient has had varicella in the past a serum sample (clotted blood) should be sent to the lab for varicella IgG. If this is positive this indicates past infection and therefore immunity. Patients with zoster will have preexisting IgG antibody. Patients with chickenpox may be positive for VZV IgM antibodies but are often seronegative at presentation. If a blood sample is sent at the onset of the rash a repeat specimen should be sent after recovery to detect seroconversion (development of IgG).
2 Direct immunofluorescence: is this varicella? The simplest and fastest way of obtaining a diagnosis of varicella is by sending a scraping from the base of a vesicle on a slide to virology, and a swab from the base of the lesion in viral transport medium for culture.
Infection control and contacts
Anyone without a past history of varicella is at risk of developing the disease after exposure. The disease can be more serious in adults, particularly those who smoke, due to the risk of varicella pneumonitis. Immunosuppressed individuals and neonates are at increased risk of haemorrhagic or disseminated varicella. There is also an increased risk of varicella pneumonitis in pregnant women, along with the risk of congenital varicella syndrome in the foetus. Congenital varicella syndrome includes limb hypoplasia and skin scarring, microcephaly, cataracts and growth retardation. The risks to the foetus have been estimated to be less than 1% in the first 12 weeks pregnancy and approximately 2% between weeks 13 and 20. After this gestation maternal infection may cause herpes zoster in the infant, up to the week before and after delivery when infection can be severe or fatal in the infant.
First determine whether contact occurred in the infectious period (see above). Pregnant women whose immune status is unknown should have an urgent VZIgG assay requested (obtain advice from the lab). This can be done the same day by the lab if necessary. Human varicella zoster immunoglobulin (VZIG) is recommended as prophylaxis for individuals fulfilling all of the following three criteria.
(a) a clinical condition which increases the risk of severe varicella e.g. immunosuppression, pregnancy, neonates
(b) no antibodies to varicella
(c) significant exposure to chickenpox or herpes zoster
VZIG is obtained from the virology department and is only effective if given within 10 days of exposure, preferably within 72 hours. It does not prevent infection but may attenuate disease.
Healthcare workers without varicella antibodies should not have contact with patients during their incubation period, returning to work 21 days after exposure. Individuals who have received VZIG have longer incubation periods. Ideally the immune status of immunocompromised patients should have been checked and susceptible individuals should be immunised and advised to avoid contact with infected individuals.
Apart from the issue of timing of the contact, as described earlier, the type of contact and closeness and duration of contact are important. The need for VZIG is restricted to those in contact with chicken pox, disseminated zoster, immunocompetent individuals with exposed lesions (e.g. ophthalmic zoster) or immunosuppressed individuals with lesions anywhere (viral shedding may be greater). A significant duration of contact would be 30 mins or more within the same room, or face-to-face contact e.g. having a conversation. Transmission from household contacts is particularly efficient.
To obtain VZIG contact your local virology department for advice. It will either be issued from the department itself or from Public Health Laboratories and the Communicable Disease Surveillance Centre (CDSC).
In the UK varicella vaccine is available privately but the UK's immunisation body decided against universal vaccination of children. Patients not immune to chickenpox who are at risk of complications from varicella if they are exposed may discuss vaccination. It may also be recommended for healthcare workers and close contacts of immunosuppressed who are not already immune. The vaccine is given as two separate injections, usually into the upper arm, four to eight weeks apart. The varicella vaccine is effective in making about 90% immune. The vaccination cannot be given in pregnancy and pregnancy should be avoided for 3 months after the injection.
Management of chicken pox
Children: it is a self-limiting illness and management is supportive. They should avoid pregnant women and immunosuppressed patients (but, not necessarily other children). Aspirin should not be given due to the risk of Reye’s syndrome, a syndrome of encephalopathy and liver damage associated with varicella and influenza. Topical antipruritics such as Calamine lotion are very old fashioned but do seem to afford relief from itch. A mild antihistamine may be advised.
Adults: treatment is also supportive, but they should be monitored for complications of varicella. Treatment with aciclovir is indicated for otherwise healthy adults presenting within 24 hours of the rash who smoke and/or have chronic lung disease and pregnant women in the second half of pregnancy. Treatment is also indicated in adults who develop respiratory symptoms and a fever (may require intravenous therapy therefore seek specialist advice- there is also a risk of permanent lung fibrosis).
• Secondary bacterial infection of skin
- Viral pneumonia occurs in 1 in 200 adults (compare with 1 in 200,000 children) 10% smokers increased risk in immunocompromised individuals and pregnancy.
- Haemorrhagic chicken pox. Lesions may appear purpuric. May be associated with thrombocytopenia and disseminated intravascular coagulation so seek specialist advice.
- Encephalitis cerebellar ataxia in children- most recover fully but it may take months. More common in immunocompromised. 3-4/100,000 cases in children.
Management of Shingles
Early treatment with high dose acicilovir (800mg orally 5 times per day) has been shown to reduce zoster-associated pain, produce faster resolution of the rash and decrease eye complications. Oral famciclovir (dose 250mg three times tds) seems to be as effective. There is some evidence that low dose amitryptiline given early also helps reduce intensity and duration of pain. Prednisolone given acutely with aciclovir reduces acute symptoms but does not seem to shorten duration of zoster associated pain (ZAP). Sympathetic nerve blocks have been reported anecdotally to reduce ZAP. Mild opiate analgesics will provide relief during the acute attack. Furthermore, gabapentin, a GABA analogue has been shown to reduce pain of three months duration. Carbamazepine should not be used- this is effective in trigeminal neuralgia, not herpetic neuralgia. Acupuncture may provide pain relief for some patients, along with topical measures such as ice packs and capsaicin. Patients with intractable pain may benefit from referral to a specialist pain clinic.
Primary herpes simplex infection
Clinical Tip: With Herpes Infections look for lesions in groups/clusters. Lesions are monomorphic usually (unless secondarily infected).
Primary herpes infections can cause
- Gingivostomatitis: infection may involve the buccal and gingival mucosa, tongue and fauces. Vesicles evolve into shallow painful ulcers on an erythematous base; they may coalesce if extensive. Other features include fever, submandibular lymphadenopathy, febrile convulsions in children and abnormal liver function tests. The lymphadenopathy may persist for several weeks after the ulcers have healed. Conjunctivitis, myalgia, abdominal discomfort and pharyngitis may also occur. Oral disease may be associated with lesions elsewhere, possibly caused by autoinoculation from the site of primary infection. The incubation period is 2-12 days and illness duration is usually 2-3 weeks.
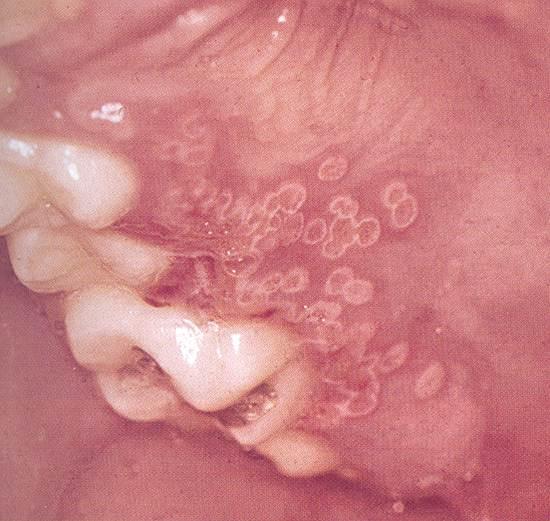
Note clustered monomorphic lesions
- Genital infection: the lesions are located principally on the vulva in women and may extend to the perineum, upper thighs and buttocks. In men, vesicular lesions are seen on the glans penis or penile shaft. Secondary bacterial infections may occur, requiring antibiotic therapy. Sacral radiculitis, associated with urinary retention and neuralgia may occur. Primary genital infection is associated with fever, dysuria, urethritis, inguinal lymphadenopathy and malaise, and lasts up to 3 weeks. Recurrent genital herpes may occur with more scanty vesicular lesions associated with localised irritation rather than significant pain. New vesicles may occur after the initial lesions have crusted over, delaying healing. Complications are rare with recurrent infection.

Clinical Tip; Complex, multi-site or slow to resolve perianal or gential HSV should alert you to the possibility of underlying HIV infection
- Eczema herpeticum/ kaposi’s varicelliform eruption: a superinfection of eczematous skin, especially in young children. There are usually systemic symptoms such as fever and lymphadenopathy. As these patients are often on steroid treatment this facilitates the spread of the virus, and untreated this condition has a significant fatality rate. Patients should be advised to take care with close contact with relatives with coldsores.
Clinical Tip- Look for groups of monomorphic punched out lesions. Don't expect to see intact blisters.
- Herpetic whitlow: an inflammation at the nail fold due to direct inoculation of the virus into the fingers through a portal of infection. This is common in health care workers especially those involved with manipulation in the mouth (e.g. anaesthetists, dentists), but may also been in nailbiters and workers such as laboratory personnel who sustain a traumatic injury with contaminated needles or glassware. The whitlow is extremely painful and takes about four weeks to heal.

Herpetic whitlow. Can be differentiated from dactylitis by the presence of grouped clustered vesicles
- Conjunctivitis and keratitis: both the conjunctiva and cornea may be involved and there may be visible vesicles and ulcers on the eyelids.
- Erythema multiforme (EM). Mycoplasma pneumonia and HSV are the infectious agents most commonly recognised as precipitants of EM. Erythema multiforme does not respond to aciclovir but recurrent cases can be prevented by prophylactic acyclovir. Sometime in more severe EM it may be necessary to treat with oral steroids.

Erythema multiforme- typical acrally distributed targetoid lesions

Typical cold sore of HSV1

Vesicles in Herpes simplex infection- note the typical clustering
HSV in the immunocompromised
Infection begins usually in either the oral or genital sites and can progress rapidly to extensive ulceration. Cutaneous dissemination may make the rash look like varicella. There is also a risk of visceral dissemination causing encephalitis, pneumonia and hepatitis. In patients with HIV recurrent infection may occur at multiple sites with high frequency and the lesions may be slow to resolve.
The virus establishes a latent infection of dorsal root ganglia, the trigeminal ganglia for HSV-1 and the sacral ganglia for HSV-2. Reactivation of the virus produces recurrent infection. The triggering process is not understood but a variety of stimuli have been implicated: common cold, sunlight/ ultraviolet light exposure, stress, menstruation, infection and mild trauma. Severe primary infections are associated with a higher frequency of reactivation.
As for varicella zoster, the simplest method to make a diagnosis is to send a scraping from the base of a vesicle on a slide to virology, and a swab from the base of the lesion in viral transport medium for culture. Type specific varicella antibody detection is not generally useful, but may be performed in special cases after discussion with the virology lab e.g. repeatedly culture negative lesions which appear clinically to be HSV.
Primary HSV1 is often mild and symptomatic treatment may be all that is needed e.g. chlorhexidine mouthwashes and simple analgesia in the case of gingivostomatitis. Primary HSV2 infection may be more severe and is more likely to present with fever. In severe cases oral aciclovir, valaciclovir or famciclovir is recommended. Steroid treatment should be withheld or reduced as it increases the severity of the disease, although as mentioned earlier it is sometimes used in more widespread EM. Aciclovir cream may be useful in the treatment of recurrent infection but the most effective treatment for severe recurrent infections is a 5-day course of oral acyclovir commenced when prodromal symptoms begin. Patients with frequent recurrences should be considered for continuous suppressive therapy.
Primary infection during the first and second trimester of pregnancy is not associated with a significant risk to the foetus. Most cases of neonatal herpes occur as a result of perinatal infection. Infection in the third trimester is associated with a risk of transmission to the baby during vaginal delivery and risk is highest when infection occurs around the time of delivery. The mothers of most infants who develop neonatal herpes do not have genital lesions at delivery. Primary genital herpes poses the greatest risk but there is also a risk with recurrent infection. A few cases occur due to transfer of the virus from oral lesions to the infant post delivery. Most cases are due to HSV-2, but HSV-1 can also cause neonatal herpes. Symptoms appear 4-5 days post partum, with evidence of skin, eye and mouth infection. The infant may also develop encephalitis and disseminated disease involving lung, liver, adrenals, eyes and skin. Mortality is greater than 80% for disseminated disease, without treatment. Most babies exhibiting only skin, eye and mouth involvement will develop permanent ocular damage and eventually show some evidence of neurological impairment. All HSV infections identified in the neonatal period should be treated with an antiviral agent. Caesarian section is recommended if clinically apparent cervical infection is present at parturition; delivery by either vaginal or Caesarian should be rapid to minimise exposure.
Other viral causes of vescicular rashes
• Coxsackie viruses can cause herpangina and hand, foot and mouth disease.
Herpangina is characterised by a painful eruption of vesicles in the mouth and throat, including the soft palate (unlike herpes simplex), fever and abdominal symptoms. It is commonest in children aged 2-10 years and is self limiting.
Hand, foot and mouth disease consists of an ulcerative exanthem of the buccal mucosa, mild fever followed by painful vesicular lesions on the hands or feet. It may spread within families and is also self limiting. Sometimes the lesions look more like a little paper cut on a base of erythema.

Vesicles on sole in Hand foot and mouth disease
• Parapoxviruses: can cause orf, a contagious pustular dermatitis contracted from sheep and goats, and paravaccinia (pseudocowpox, ring sores) which is contracted from cattle. Infection is localised and occurs via cuts and abrasions. Lesions start as erythematous papules and progress to a ‘target’ lesion 1-2 weeks after infection, appearing as a red centre surrounded by a white halo and an outer erythematous halo. The lesion then becomes nodular and then papillomatous, often with a weeping surface, and resolves over a period of weeks with crusting. Occasionally lesions become large and granulomatous, needing surgical removal. Vesicles are occasionally visible to the naked eye, but the lesion generally does not look classically vesicular. Most patients have a single lesion only, which is mildly painful. The patient is normally systemically well although lymphadenopathy and malaise may occur. Diagnosis is clinical, but samples of the lesion may be sent to the virology lab for detection of the virus using electron microscopy. Infection may spread between human contacts, so patients should be advised to avoid spreading the infection by contact with broken skin.

Maculopapular rashes may arise following infection with any of the following:
- Rubella
- Parvovirus
- Entero/Echovirus
- Measles
- EBV
- CMV
- Dengue
Viral causes of a maculopapular rash according to age group
| Age <1 year | 1-5 years | 5-10years | 10-15years | Adults |
| HHV6 | HHV6 | Parvovirus | EBV | Rubella |
| Rubella | Rubella | Rubella | CMV | Parvovirus |
| Measles | Measles | Rubella | ||
| Parvovirus |
Parvovirus infection 'Slapped cheek'
50% infections are asymptomatic. Otherwise there is commonly a biphasic illness consisting of a brief prodrome of a non-specific febrile illness with a cough, followed by recovery and approximately seven symptom free days. Then the classical fiery red, macular ‘slapped cheek’ rash develops which spares the area around the mouth (circumoral pallor) and has slightly raised edges. The rash spreads 1-4 days later to involve the trunk and limbs and becomes maculopapular, resolving with central clearing to form a lacy (reticular) pattern. It is most prominent on extensor surfaces and is itchy. It rarely affects the palms or the soles and can look very similar to rubella. It lasts 1-3 weeks and fluctuates with environmental factors e.g. it may flare after a hot bath.
Caused by Parvovirus B19 it is spread by droplets. It is usually benign but may cause the following problems:
- Joint involvement is rare in children but common in adult females (80% infections with a rash). In this group joint arthritis may occur without a rash, and is commonly a sudden onset symmetrical arthritis affecting the small joints of the hand, usually the proximal interphalangeal joints (PIPs). The arthritis usually resolves within 4 months.
- Aplastic crises may occur in patients with chronic haemolytic anaemia e.g. sickle cell disease. There is a sudden fall in haemoglobin which may last 5-7 days due to a lack of red cell precursors (reticulocyte count will be low). The patient will present with symptoms of anaemia.
- Chronic anaemia may occur in immunocompromised patients who have failed to produce neutralising antibodies and have chronic parvovirus infection. The anaemia resolves after administration of Normal Human Immunoglobulin (NHIG) and these patients may develop a rash illness subsequently, due to the deposition of immune complexes.
- There is no evidence that parvovirus causes birth defects. However, foetal hydrops may occur due to 2nd or 3rd trimester infection and may occur from 2-12 weeks after the rash. For this reason women who have had parvovirus infection in pregnancy should be monitored closely to assess the development of hydrops in the foetus. Such babies may require foetal exchange transfusions. Termination is not advised if there is no evidence of hydrops and the pregnancy is proceeding normally but specialist advice should be sought. Miscarriage has been reported in the first trimester following contact with B19.
Diagnosis is usually clinical but if necessary a clotted blood sample can be sent for the detection of parvovirus specific IgM (indicating current infection) and IgG (indicating previous/current infection). Ideally a blood sample should also be sent from the index case to confirm parvovirus infection. In the case of immunocompromised patients the virus can be detected using PCR to detect viral DNA in the serum.
B19 can also cause the Purpuric Glove and Stocking eruption in adults.

Slapped cheek
Rubella
Infection may be asymptomatic in up to 25%. Adults may experience prodromal symptoms of malaise and fever for a day or two before the rash but in children the onset is usually abrupt, with the appearance of the rash. The rash starts on the face as macular lesions and then spreads to the trunk and limbs. It seldom lasts for more than 3 days and may also be seen on the soft palate. There is usually pharyngitis and enlargement of the cervical, and especially the suboccipital and postauricular lymph nodes. Lymphadenopathy may be generalised and tender, may present up to a week before the rash and persist for 10-14 days after the rash. Constitutional symptoms are usually mild in children. N.B. the rash is not diagnostic of rubella as other viruses may cause the symptoms.
Clinical tip: the rash is often a very specific 'pillar box' red in colour and look for occipital lymph nodes.
It is usually benign but the following complications are recognised
- Arthralgia- rare in children but may occur in up to 50% of adult females. It usually develops as the rash subsides and persists for less than a week (occasionally longer). The most common joints affected are the finger joints, wrists, knees and ankles. The arthralgia is believed to be mediated by immune complexes but hormonal factors may play a role because in female vaccinees joint symptoms are most likely to develop within 7 days of the onset of the menstrual cycle.
- Postinfectious encephalomyelitis may develop in 1 in 5000-10,000 cases within a week of onset of the rash. It is not associated with demyelination or inflammatory damage and the prognosis is good.
- Thrombocytopenic purpura is rare.
- Primary maternal rubella infection in the first ten weeks of pregnancy results in foetal damage in up to 90% of infants. The risk of damage declines to 10-20% by 16 weeks and is rare after 16 weeks. Congenital rubella syndrome consists most commonly of a triad of cardiac abnormalities (e.g. patent ductus arteriosus, ventricular septal defect), cataracts and deafness. Other abnormalities include mental retardation, growth retardation, hepatosplenomegaly, jaundice, anaemia, thrombocytopaenic purpura and bony lesions. Any combination of defects may occur, although perceptive deafness and pigmentary retinopathy may occur alone. Infants may appear normal at birth. Rubella re-infection has a lower risk of foetal infection, approximately 8% in the first 16 weeks of pregnancy, and foetal malformations are rare. Infants with congenital rubella syndrome are highly infectious, excreting virus from their pharynx and in urine. Approximately one third will still excrete virus at 6 months of age, although this seems to be rare after the age of 2 years.

There is good immunity after both naturally acquired rubella and vaccination. However, reinfection may occur and can be asymptomatic. It is diagnosed by demonstrating a significant rise in specific anti-rubella IgG following exposure.
All pregnant women with possible rubella infection or exposure to rubella need to be investigated serologically regardless of a history of previous rubella or vaccination. Blood should be taken as soon as possible after the onset of symptoms or exposure to detect the presence of rubella specific IgG and IgM. No particular titre of antibody is indicative of present or recent infection-a further sample should be sent 7-10 days later to detect a significant rise in antibody titres. Low levels of IgM may be detected for up to 4 years following rubella vaccination and may be detected in reinfection so this result is not diagnostic of recent primary infection. A good clinical history of LMP, timing of exposure, symptoms and previous infection/ vaccination will help in the interpretation of the results. Sending a blood sample for detection of rubella IgM or a salivary swab if the case is a child should do confirmation of rubella in the index case.
The vaccine consists of live attenuated virus and is therefore not recommended in pregnancy. Susceptible women should be vaccinated after delivery. Pregnancy should be avoided for one month after rubella vaccination.
Post exposure prophylaxis with HNIG is of little value as it does not prevent infection in non-immune contacts, although it may reduce the likelihood of clinical symptoms. Its only recommended use is for when termination for confirmed rubella would be unacceptable, and it should be given soon after exposure.
Other viruses which cause rubelliform rashes and arthralgia
Parvovirus B19, enteroviruses (coxsackie A, echovirus) and some arboviruses e.g. Ross River virus.
Measles
Prodromal symptoms are respiratory and usually consist of fever, malaise, rhinitis, conjunctivitis and cough. The patient is highly infectious at this stage. Koplik’s spots may appear on the buccal mucosa inside the cheek and mouth; these tend to fade as the rash begins. The main illness consists of fever and a dusky red maculopapular rash which starts on the forehead and behind the ears and spreads to the rest of the body. It fades to a brownish colour and resolves with fine desquamation. It is not itchy. Generally, the fever, conjunctivitis and respiratory symptoms subside when the rash is at its peak.
The incubation period is approximately 10 days, the prodrome lasts 2-4 days and the rash appears approximately 2 weeks post exposure. Spread is via the respiratory route. Patients are infectious from the beginning of the prodrome until four days after the appearance of the rash. The incidence increases in winter and early spring.

Kopliks spots in buccal mucosa
Complications of measles
- Opportunistic infections can occur, particularly bronchopneumonia, croup and otitis media.
- Giant cell pneumonia: rare, usually only in immunodeficient or with chronic debilitating disease. It is caused directly by measles virus and is very severe.
- Measles inclusion body encephalitis: only in immunosuppressed, presents with convulsions, myoclonic jerks, coma and stupor. Death occurs within weeks or months; the course is more rapid than subacute sclerosing panencephalitis (SSPE).
- Acute measles postinfectious encephalitis: occurs in 1 in 1000-5000 cases of acute measles and 20-40% have lasting neurological sequelae such as fits, hemiplegia and mental retardation. It develops with fever, headache, seizures, cerebellar ataxia and coma. The mortality rate is 15%.
- Subacute sclerosing panencephalitis (SSPE): usually occurs in children and young adults 6-8 years after acute measles and has an incidence 1 per million cases. It is commonest in children who had measles before the age of 2 years. The illness lasts 13 years and leads to death. It is characterised by generalised intellectual and psychological deterioration, fits, aphasia, myoclonic jerks and chorioretinitis. There are characteristic EEG changes. It is due to persistent measles infection and patients have high titres of anti-measles IgG and IgM in serum and CSF.
- Other complications include hepatitis, myocarditis, pericarditis and mesenteric lymphadenitis.
- Case fatality rates for measles are age related- high under the age of 1year, lowest for the age group 1-9years, then increasing with age.
A saliva sample should be sent for specific measles IgM, ideally 3 days after the onset of the rash. A blood sample may be sent at the time of diagnosis, for the detection of measles specific IgM, followed by a further sample 7-10 days later to detect a rise in antibody titre.
Contact with measles poses a risk for children under the age of 1year, the immunocompromised, and those with chronic debilitating disease. Parents who do not remember either having measles or being vaccinated are also at risk. It is therefore of importance that these individuals be immunised. Susceptible individuals at risk may be protected after exposure by the administration of human normal immunoglobulin, given within 3 days of exposure. Effectiveness disappears if given greater than 6 days after exposure.
The illness is normally self-limiting, but complications such as bacterial infection will need to be treated with antibiotics. More severe complications will obviously necessitate referral to hospital.
Roseola infantum
Caused by Human Herpes Virus 6 (HHV6)
Primary HHV6 infection usually manifests in children as an acute febrile illness lasting 3-4 days; 10% will also have a macular or papular rash on the face and trunk similar to measles or rubella (it is commonly misdiagnosed). Transmission is via salivary secretions. Complications include febrile seizures, hepatitis, bone marrow suppression, encephalitis, gastrointestinal symptoms and respiratory symptoms (pneumonitis in 10%). HHV6 infection accounts for a third of febrile seizures under the age of 3 years.
The diagnosis is generally clinical, but in some circumstances (e.g. child with neurological complications) indirect immunofluoresence and PCR can be used to identify the virus. These investigations are generally done by a reference lab and need to be discussed in advance.
Other main causative agents of a maculopapular rash
Both Epstein-Barr virus (EBV) and Cytomegalovirus (CMV) can cause infectious mononucleosis. The seropositivity of EBV increases with age, with greater than 90% of adults worldwide being seropositive: conversely, primary EBV is unusual in the middle aged and elderly. There are two age groups in whom infection peaks; 1-6 years and 14-20 years.
EBV infection
It may be subclinical in healthy adults (50% infections) or present abruptly with a painful throat, fever, malaise, headaches, neck stiffness, anorexia and vague abdominal discomfort. Palatal petechiae occur in the first week of illness, and they may be associated with a greyish membrane and exudative tonsillitis. Two types of rashes are seen; a generalised, faint, non-itchy morbilliform rash lasting under 2 days, and a florid maculopapular rash seen in patients given penicillin. Generalised lymphadenopathy occurs, the nodes being palpable for several weeks. Splenic enlargement occurs in 50% patients and hepatomegaly, mild jaundice and derangement of liver function also occurs in a significant proportion of cases.
Close contact: the virus is present in salivary secretions. The incubation period is 30-50 days.
Complications
- Pharyngeal oedema and tonsillar enlargement can result in obstruction of the pharynx or trachea.
- Splenic rupture is very rare.
- Neurological complications such as meningitis, encephalitis or Guillain-Barre syndrome may precede, accompany or post-date Infectious mononucleosis by weeks.
- Hepatic complications: jaundice occurs in 5-10%.
- Chronic cases can occur where symptoms persist for greater than 1 year (approx 1 in 2000) cases. The average duration of symptoms is 2-3 weeks.
- Immunological complications include haemolytic or aplastic anaemia, thrombocytopaenia, agranulocytosis and hypogammaglobulinaemia.
Clinical Tip: Affected individuals should be warned to avoid contact sports for at least 6 months following infection if their LFTS are abnormal due to the risk of splenic rupture if kicked etc.
Diagnosis is made by full history and in the interpretation of any investigations
- Blood film: the presence of atypical lymphocytes is highly suggestive, although they are also seen in CMV infection, hepatitis B, influenza B and rubella.
- Monospot: detects IgM heterophile antibodies which cause haemagglutination of erythrocytes from species other than humans (sheep are usually used).
- EBV VCA IgM (viral capsid antigen): demonstration of IgM antibodies is diagnostic of recent infection. Demonstration of IgG antibodies is not usually helpful as they are usually present in the first serum sample taken after diagnosis.
Treatment is supportive; analgesia for the painful throat and paracetamol for fevers. Obviously penicillin should be avoided.
Pityriasis Rosea and HHV6/HHV7
There is increasing evidence that Pityriasis Rosea is associated with HHV6 and 7 infection. It most commonly affects ages 15-30 and starts with the typical 'herald patch' usually the trunk. The hallmark is the erythematous macule with peripheral collarette scale which follows on the trunk, often following the lines of the ribs (the so-called Christmas Tree distribution). This is best seen if you stand a little way back from the patient and observe the back of the chest from a slight distance. Rash may be a little itchy but usually asymptomatic. My old boss used to tell me it lasted Forty days and Forty nights!!
It doesn't usually need treatment although a mid strength topical steroid may relieve lesions and very rarely I prescribe narrow band UVB for protracted cases. Occasionally an inverse pattern can occur.
Clinical Tip: Look for Christmas Tree pattern and be aware that secondary syphilis may mimic Pityriasis rosea.


Pityriasis rosea- note typical Herald Patch and Christmas tree distribution following ribs
Cytomegalovirus ( CMV)
Clinical presentation is similar to above but the majority of cases in otherwise healthy adults are asymptomatic.
Incubation is 4-8 weeks for a primary infection. Transmission can occur via saliva, sexually (particularly homosexual men) and more rarely from blood transfusion or organ transplantation. It is also transmitted perinatally via swallowed genital secretions and breast milk, and can occur as a congenital infection.
Primary CMV infection in the first 28 weeks of pregnancy causes a risk of cytomegalic inclusion disease in the foetus of about 4%. However, the presence of intrauterine infection does not necessarily cause clinically evident disease in the infant, the majority of these infants developing normally. These cases are difficult and should be discussed with the virologist and obstetrician. Ultrasound scanning and amniotic fluid testing for CMV may help identify potentially damaged cases. In the case of pregnant healthcare workers exposed to infectious CMV cases there is little evidence that they have an increased risk of developing infection, but good hygienic measures should be advised.
Symptomatic infants are described as having the syndrome of ‘cytomegalic inclusion disease’ which includes intrauterine growth retardation, jaundice, hepatosplenomegaly, thrombocytopenia, encephalitis, microcephaly, pneumonitis, myocarditis, hepatitis and congenital abnormalities of the 1st branchial arch and anophthalmia. Of those infected, 7% will be symptomatic at birth and 1% will die in infancy. Those which survive suffer fits, spastic diplegia, perceptual organ damage such as optic atrophy and deafness, and mental retardation. Of those infants which are asymptomatic at birth 15% will have hearing defects and/or mental retardation. Congenitally infected infants excrete CMV in urine, saliva and nasal secretions and so care should be taken to avoid close contact with pregnant women.
Diagnosis
The virus can be isolated from urine samples and saliva soaked into a cotton tipped swab sent in viral transport medium. Virus can be more rapidly detected in urine using the DEAFF test. The presence of CMV IGM in an acute blood sample is diagnostic of recent infection. PCR of plasma, whole blood and lymphocytes can be used to diagnose systemic viraemia. This is useful in monitoring immunosuppressed patients on therapy.
Again, management is supportive. Antiviral therapy is only indicated for serious or life-threatening CMV infection in the immunocompromised.
- Coxsackie A and echovirus can cause a fine rubella-like rash. It may be associated with fever, malaise and cervical lymphadenopathy and recovery is usually uneventful.
- Dengue virus often causes a diffuse, discrete maculopapular rash, heralding the recovery phase of dengue fever.
WARTS
These are predominantly caused by
- Poxviruses
- Papilloma viruses
Warts are caused by Human Papilloma viruses (HPV) which infect and replicate in squamous epithelium. They enter the skin through small abrasions. The incubation period is probably a matter of months.
Common warts: firm papules with a rough horny surface. They are commonest over the knuckles and nail folds, and can also occur on the knees and on the shaft of the penis. They are caused by HPV 1,2 +4.

Common warts on fingers
- Plantar warts (verrucae) generally occur at pressure points. They start as a small papule and as they enlarge small thrombosed capillaries may be seen in the tips of the elongated papillae.
- Plane warts: smooth, flat or slightly elevated, occurring on the face or the back of the hands. They may form lesions at the site of abrasions (Koebner’s phenomenon). They are caused by HPV 3 +5.

Plane warts
- Filiform warts are common in the beard area, on the lips and in the nasal vestibule.

- Mosaic warts consist of clusters of small warts.
- Benign condylomata (genital warts) are caused by HPV-6 and 11. Classical genital warts are multiple, pointed, and fissured. In women they occur most commonly at the posterior introitus and adjacent labia; also the vulva, perineum, vaginal wall and cervix (a smear should be taken). Warts enlarge during pregnancy and may occasionally obstruct the vagina. In men warts may occur on the frenum, coronal sulcus or glans. Intrameatal warts may spread into the urethra. Perianal warts may spread into the anal canal. They can occur in both homosexual and heterosexual men. HPV 16 +18 appear to risk factors for genital malignancy, and are found in approximately a third of malignancies. However, note that direct transformation from wart to malignancy appears to be very rare. HPV can also be found in cells from a normal cervix. In the UK a recently introduced vaccination programme for 13+ year old girls is aiming to reduce cervical cancer rates by prevention of HPV infection.

Treatment
Most will resolve spontaneously. Genital warts regress less frequently than skin warts.
There are a wide variety of treatments for warts as below. The best evidence base exist for either salicylic acid or cryotherapy. I often try and persuade patients to do nothing if possible!!
- Salicylic acid 20-40% is effective when applied as a paint or plaster after soaking the skin for 5 mins with warm water. The surrounding skin should be protected with a ring of vaseline
- Cryotherapy may be used without anaesthesia but is often not practical for large warts.
- Formalin 10% can be used as a soak for multiple warts on the soles of the feet.
- Fluouracil 5% cream or solution (Efudix®) may be used either alone or alternating with topical retinoids in the treatment of plane warts.
- Podophyllin 10-20% in liquid paraffin may be painted onto anogenital warts and the area then powdered. The coating may be washed off 3-4 hours later. The treatment is repeated 1-3 weekly. It can be irritant and should not be used in pregnancy due to the risk of systemic absorption and damage to the foetus. It should also not be used on the cervix, because of the risk of neoplastic change. If a local reaction occurs the treatment should be stopped and 1% hydrocortisone applied topically twice daily until the inflammation has resolved. The treatment can then be tried again with caution.
- Imiquimod (5%), an immunomodulator, has recently been introduced for genital warts, and trials are ongoing in cutaneous warts.
- Electrocautery may be used for some types of warts but must be done using local anaesthesia.
- Surgical excision may occasionally be used to remove or debulk extensive warts, especially perianal warts.
- Laser evaporation using a carbon dioxide laser can be used for both mucosal and cutaneous lesions.
- Loop electrosurgical excision procedure (LEEP) uses a heated loop to remove cervical lesions. The lesions is removed intact and can be sent for pathological examination
- There is evidence against using Cimetidine.
Molluscum contagiosum
It is caused by a poxvirus and is transmitted from person-to-person and via close body contact. School children are particularly susceptible. Infection occurs through abrasions of the skin.

Molluscum contagiosum – umbilicated, firm white papules. Note the apparent inflammation and 'impetiginisation' which often heralds spontaneous clearing of lesions
The characteristic lesions are small, smooth pearly-white or flesh coloured umbilicated papules which become dome shaped. They vary in size from 1–5 mm and occur commonly on the face, hands, arms, abdomen, buttocks and genitals. They are rare inside the mouth or on the soles of the feet. They may become confluent along lines of abrasions. They can be transmitted to other areas of the body by autoinoculation.
Clinical tip: Giant molluscum in an adult should alert you to a possible underlying HIV infection
Treatment may be sought for cosmetic reasons, particularly for facial lesions. A proprietary preparation containing 5% potassium hydroxide is available in the UK and may lead to resolution of lesions after 4-6 days.
Mucocutaneous lesions caused by viruses
| Virus | Lesion | Virus shedding? | |
| No Systemic Spread |
Papilloma |
Common wart Plantar wart Genital wart |
Yes |
|
Molluscum Contagiosum |
Smooth umbillicated fleshy papule |
Yes | |
| Orf | Papulovesicular | Yes | |
| Systemic spread |
Herpes simplex Varicella zoster |
Vesicular |
Yes |
|
Coxsackie A |
Vesicular, mouth (herpangina) |
Yes | |
|
Coxsackie A16 |
Vesicular (hand, foot and mouth) |
Yes | |
|
Parvovirus B19 |
Facial maculopapular |
No | |
|
HHV6 |
Exanthem subitum (roseola infantum) |
No | |
|
Measles |
Maculopapular |
No | |
| Rubella |
Maculopapular |
No | |
|
Echoviruses |
Maculopapular |
No |
FUNGAL DISEASES
Fungal infections are tremendously common in dermatological practice but even so we regularly joke that dermatologists often miss the diagnosis of tinea!!
Essentially two types of pathogens cause trouble on the skin:
- Yeasts e.g. candidiasis and seborrhoeic dermatitis.
- Moulds e.g. ringworm and fungal nail infections
Fungal infections
These can be considered as below:
- Superficial mycoses. Very common e.g. 20% people with tinea unguum/pedis
- Deep mycosis. These are uncommon in the UK but more common in the tropics.
- Systemic mycoses. Rare except in immunocompromised. Candida and malassezia species may be part of the normal flora but can cause disease in susceptible individuals
Candidal infections
There are several species, of which the commonest is candida albicans. These are usually superficial infections which thrive in hot sweaty areas. Typically they cause problems as below:
- vulvovaginal (thrush), oral, intertrigo, balanitis, napkin dermatitis
- risk factors: diabetes, pregnancy, immunosuppression
- treat with topical antifungals, e.g. imidazole e.g. polyenes (e.g. nystatin); can treat with oral imidazoles (e.g. fluconazole) if necessary

Candidal intertrigo- note satellite lesions which can help with diagnosis
Candidal nail infection
Clinically this presents with onycholysis, paronychia, dystrophy. May be seen in patients with Raynauds, Cushings, or in people who immerse the hands in water for prolonged periods. Treatment is with oral imidazoles, and advice regarding hand care and avoiding excess moisture.

Chronic paronychia – candida
Chronic mucocutaneous candidosis is rare familial condition which usually presents in childhood with recurrent oral candida and paronychia,
Clinical Tip- Candida and moulds tend to cause paronychia and a lot of inflammation in the periungum
Amorolfine may be helpful for topical therapy of candida , although it is not very efficacious generally. Needs to be used for up to 12 months.
Malassezia yeast infections
Malassezia furfur is a normal skin flora, previously called pityrosporum species. It commonly presents with problems especially in atopics and immunosuppressed. There are various patterns of infection:
- Seborrhoeic dermatitis – scaling of scalp and face ‘T’ zone-characteristically orange -red hue. Also caused napkin dermatitis.
- Pityriasis versicolor –see below
- Pityrosporum folliculitis – itchy, back and upper trunk in young males- see above.
Pityriasis versicolor
This is a very common rash usually seen in teenagers. Patients usually complain about it when they come back from a holiday and find that the rash is more noticeable when as it didn't tan! Typically we see coalescent orange- brown patches with surface scaling which can be helpful when making the diagnosis. Woods lamp shows pale yellow fluorescence though in reality one doesn't need to use this to make a diagnosis. Slight hyperkeratosis causes brownish colour in white skin, whereas the azaleic acid produced by the yeast causes hypopigmentation in dark skin. Hence the name- versicolor (variable colour).
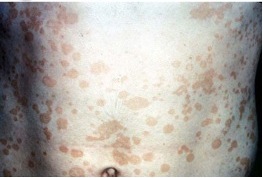
Pityriasis versicolor – oval hyperpigmented patches
Treatment is with topical antifungals e.g. selenium sulphide (Selsun®) shampoo e.g. ketoconazole (Nizoral®) shampoo or cream e.g. terbinafine (Lamisil®). Occasionally I prescribe oral imidazoles e.g. itraconazole (NOT ORAL TERBINAFINE) if severe or resistant disease. Hypopigmentation persists for months and may become more obvious with a subsequent tan. Warn patients about this!!
Clinical tip: Flaking on scratching the lesions helps confirm the diagnosis
DISEASES CAUSED BY MOULDS
Moulds represent a large group of organisms, most of which are non-pathogenic. Human disease is caused by both dermatophytes and the non-dermatophytes
Dermatophytes = ringworm. There are 3 groups: trichophyton, microsporum and epidermophyton.
Non-dermatophytes = many types of less importance.
Presentation
These are classified according to body part affected e.g. Tinea corporis, tinea capitis, tinea cruris, tinea pedis, tinea unguium. Infection may cross anatomical boundaries, and features are related to the degree of inflammation, which in turn depends on the dermatophyte species e.g. animal species more inflammatory than ‘human’ species.

Tinea cruris – note the well-defined, inflammatory, red edge
Top Tip: Tinea in feet may be a portal of entry for cellulitis
Key features of fungal skin infection
- Well defined lesions that may have a raised edge.
- Single or unilateral.
- May have some vesicles or pustules.
- May look psoriasiform on legs and feet.
- Differentials include discoid eczema, pityriasis rosea with herald patch, lichen simplex, erythrasma.
- May be modified by steroids i.e. tinea incognito
Diagnosis is by skin scrapings for mycological culture or if available with KOH preparations in the clinic.
Treatment- small areas may be treated with topical terbinafine or ketoconazole for 2-4 weeks. In severe or widespread infection or tinea manuum use oral terbinafine or oral itraconazole for 2-4 weeks or longer for toenails - 3 months.Oral itraconazole can be used as a pulsed regime .

Tinea corporis on the arm – note the well-defined leading edge
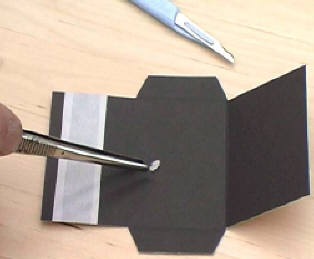
Performing skin scrapings
- Disposable scalpel or blade which is held perpendicular to skin surface
- Use Firm strokes over edge of lesion without lacerating skin
- Scrape onto black paper (easier to see).
- Fold and seal for transport.
Tinea capitis
This is a condition which is more common in children than adults and is much more common in Afro-Caribbean children. There are two common patterns, but it may be very varied in its presentation, from subtle scaling to broken 'black-dot' hairs.
It may cause a patchy rather moth-eaten alopecia –with well defined round areas of hair loss, minimal scale and broken hairs

Tinea capitis – patchy alopecia and scale
Tips: Hair plucks as well as scrapings should be taken. It is painless to extract hairs.
Kerion occurs due to exaggerated host response to presence of mould. Clinically we see a boggy inflamed mass, with pus, matted loose hair & scale crust and sometime associated with lymphadenopathy.
Tip: do not let the surgeons Incise and drain this- it responds to medical treatment, often with full hair regrowth (surprisingly).

Kerion – boggy inflammatory mass with alopecia
Investigation - with scrapings & plucked hair. Woods lamp limited value – only picks up some species.
Treatment -
- griseofulvin 10-20 mg/kg for 2 months has historically been used as first line but more recently many clinicians are using terbinafine half adult dose for 4 weeks as first line therapy. Ketoconazole shampoo should be used for both patient and unaffected siblings and other family members as fomite spread is a major issue with tinea capitis. Children should not need to be excluded from school for this, and it is important to warn of the possibility of an Id reaction, which occurs when treatment of inflamed dermatophyte e.g. kerion results in distant reaction. There are 2 patterns, namely a pompholyx like reaction and follicular papules on trunk and limbs. This resolves with treatment of dermatophyte infection.
Tinea unguium
There is often associated tinea pedis or tinea manuum, therefore take skin scraping as well as nail clippings. There may sometimes just be a couple of nails involved.
Tip: If all nails are affected it is less likely to be tinea and more likely to be primary nail pathology such as psoriasis
There 3 types typically described.
1. distal and lateral subungual onychomycosis (DLSO). This is the most common pattern with yellow/brown/black colour and soft subungual hyperkeratosis. It spreads proximally and other nails may be sub clinically infected. It may cause discomfort.

Extensive Tinea Unguium toe nails
2. white superficial onychomycosis (WSO). This produces powdery white discoloration of the distal nail and is more common in HIV disease but is also found in health adults and children.
3. proximal subungual onychomycosis (PSO) rare except in HIV. Proximal nailfold infection with rapid invasion and white nail without thickening.
Tip: It is worth sending clippings and subungual debris for microbiology. When moulds are involved one sees periungual inflammation
Treatment: terbinafine 250 mg daily for 6 weeks in fingernails and 12 weeks in toenails, or itraconazole pulse 400 mg/day (as 200 mg bd) for 1 week per month for 3-6 months or as 200 mg daily for 12 weeks. It has a long half life and may persist in the nail plate for up to 6 months and may cause taste disturbance which can be permanent. It has minimal drug interactions. It is better for diabetic patients and those with HIV.
Itraconazole is fungistatic but us more braid spectrum and reasonably good for candida and moulds. Pulse therapy useful as decreases risk of toxicity. Monitor LFT if long term or other hepatotoxic drugs.
If treatment is unsuccessful, reconsider diagnosis e.g. trauma, psoriasis, LP, eczema.
Elderly and patients with e.g. psoriatic nails harder to treat.
Non-dermatophyte mould infections
These are relatively uncommon in the UK but more common in some tropical countries, USA and the Mediterranean region. e.g. Scytalidium spp:
- Causes Ringworm like infections
- Affects palms, soles and webspaces
- Nails are frequently involved, including onychomycosis
- It is difficult to treat with usual oral antifungals
- It may require nail removal.
- Whitfield’s ointment can be useful for scaling sole lesions
Other fungal infections
The rest of the fungal infections are mostly subcutaneous or systemic and tend to occur in Indian subcontinent, Middle-East and Africa
Subcutaneous mycoses
These are infections caused by fungi which are directly inoculated into the dermis or subcutaneous tissue through a penetrating injury. Mainly seen in the tropics.
Sporotrichosis
Fungus is usually introduced by trauma, e.g. by a thorn or splinter, usually into the upper limb where a nodule or pustule forms and via lymphangitic spread a chain of nodules develops. Whilst it may resolve spontaneously it is usually treated with Itraconazole.

Systemic mycoses
These are fungal infections that involve deep structures and can spread, usually via the bloodstream, to a site distant from the original focus of infection.
Cryptococcus yeast in HIV infection

- often resembles molluscum contagiosum on the skin
- Systemic involvement is usual – CNS and lungs
- needs amphotericin B + imidazoles
COMMON PARASITIC INFECTIONS
Scabies
This is one of the most itchy rashes around. Diagnostic clues include
- interdigital, penile, peri-umbilical, flexures, axillae
- contact history
- crusted scabies in immobile/immunosuppressed
Clinical Tip: Itch is often out of proportion to what you see on skin - there may not be many obvious burrows etc.
Clinical Tip: nodules on the shaft of the penis are pathognomic for scabies.


Scabies – note linear burrows at typical site of wrist. Feet are commonly involved in children.

Crusted scabies – loads of mites!

Scabetic nodules – commonly seen in genital region
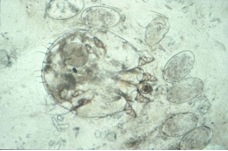
Scabies mite – isolated with needle
Treatment
Scabies - patient Information Leaflet
The Key to Success is to treat both the patient and all close contacts at the same time with two treatments a week apart, using topical Permethrin 5% cream, applied from the neck down and washed off after 12 hours, reapplying if hands are washed.
Ivermectin orally is needed for immunosuppressed or crusted scabies.
Apologies that we have covered so much this week- and even then there are a number of common infections which we have not had the opportunity to cover in depth. HIV infection will be covered later in the course.
KEY LEARNING POINTS COMMON INFECTIONS.
1. Staphylococal infections are common causes of skin disease and range from impetigo and folliculitis to staphylococcal shock syndromes.
2. Any annular lesions think of Tinea and look for tine elsewhere e.g. nails, interdigital spaces.
3. Any itchy patient think scabies!! Remember to treat both the index case and all close contacts at the same time and repeat one week later.
4. Any purpuric rash or vasculitis remember Meningococcus.
5. Wart treatment can be complicated and time consuming and ensure the treatments are not more burdensome than the condition.
Common Skin Infections
This week we will be looking at some of the more common pathogens which affect the skin in European countries. Mycobacterial disease, cutaneous manifestations of HIV disease, parasitic infestations and tropical diseases are covered in Module 5.
BACTERIAL INFECTIONS
Thanks to the introduction of antibiotics and improvements to sanitation and living conditions, bacterial infections are much less of a problem in many parts of the world than, say, 30 years ago. Nonetheless, increasing antibiotic resistance and emergence of virulent strains such as Panton- Valentin Leucocidin Staphylococci mean that these are shifting sands, and recognition and swift treatment of cutaneous bacterial infections remains as important now as then.
There are 3 key features to the development of bacterial infection:
- The integrity of the epidermis - provides a barrier to entry by bacteria. This is one reason why patients with altered barrier function in atopic eczema (and with filaggrin mutations) have such problems with staphylococcal super-colonisation and infection.
- The skin's normal bacterial (and fungal) flora prevent colonisation by pathogenic organisms.
- Host immunity.
Infection normally requires a small break in epidermal integrity to gain access such as trauma, leg ulcers, surgical wounds, IV drug user injection sites, fungal infections (e.g. athlete's foot). Also, abnormal scaling of the skin (e.g. in eczema) encourages bacterial adherence. Immunosuppression (Diabetes Mellitus, AIDS, drugs) is associated with an increased incidence of infection.
In the UK, Impetigo/cellulitis/boils (usually staphylococcal driven) are the most common infections we see, whereas in developing countries TB, Leprosy and impetigo account for most cutaneous infections.
STREPTOCOCCAL AND STAPHYLOCOCCAL INFECTIONS


Streptococcus sp Staphylococcus aureus
Impetigo
Unlike most skin disease, impetigo is a highly infectious skin disease (spread by direct contact - family/school). It is a very common condition and is most common in children. It typically presents with weeping, exudative areas with a typical honey coloured crust on the surface (esp face and hands). If you see it in an adult, you should consider whether the patient plays contact sports ('scrum pox' when spread by rugby players), has an underlying immune disorder, or whether you are seeing 'impetiginisation' of another dermatological problem i.e. secondary staphylococcal infection superimposed on a primary dermatological condition such as nummular dermatitis. It can cause blistering ("bullous impetigo") due to bacterial toxins. Over 90% of cases are caused by Staphylococcus aureus, but rarely group A Streptococci can be responsible, so taking swabs is important.


Bullous impetigo in a child. Note annular appearance Impetigo in an adult (HIV associated)
We probably overuse oral antibiotics for this condition. Localised disease can be treated with topical fucidin (three times daily) and the antiseptic povidone iodine for 1 week. In very weepy impetiginised eczema I sometimes suggest using Potassium permanganate soaks (dilute KMNO4 to pale pink solution and apply on gauze for 20 mins. Remember it stains nails and washbasins etc brown - make it up as a dilution on an old plastic bowl not the posh sink!). For more extensive disease, oral antibiotics for 7-10 days (flucloxacillin 500mg four times daily for staphylococcus; Penicillin V 500mg four times daily for streptococcus) should be used. In hospital practice we often use a combination such as CoAmoxiclav but in the community setting this practice has recently been discouraged due to the threat of increased bacterial resistance. Other close contacts should be examined and children should avoid school whilst lesions are weepy and crusty. Recurrent impetigo may occur, often due to resistant bacteria e.g. MRSA. In these cases take skin swabs for bacteria (MRSA) and check other family members. I often take nasal swabs and consider Nasal staphylococcal eradication – e.g. mupirocin (three times daily for 1 week) to eradicate nasal carriage +/-treat whole family with antibiotics/chlorhexidine. If this doesn't work, then you should consider whether there is underlying immunosuppression/diabetes.
Cellulitis
Cellulitis is a hot, sometimes tender area of confluent erythema of the skin and is usually caused by a streptococcus (occasionally staph/gram negatives). There may be a portal of entry for infection such as a recent abrasion or a venous leg ulcer. Web spaces of the toes should be examined for evidence of fungal infection. It often affects the lower leg causing an upwards spreading, hot erythema. Patients are nearly always unwell and pyrexial. It may also be seen affecting one side of the face - hot, well-demarcated swollen erythema- when it is known as Erysipelas.
Clinical Tip; Erysipelas often starts just under the eye or at the bridge of the nose and has a surprising amount of oedema. It may resemble an allergic contact dermatitis initially but the clue is that in erysipelas the patient is unwell.
Occasionally, as well as the signs described above, one can see blistering of the skin.
Diagnosis is nearly always made on clinical grounds as blood cultures are often negative. Confirmation of infection, if necessary, is best done serologically by streptococcal titres (ASOT).
In the early stages oral Penicillin or Erythromycin 500 mg twice daily (bd) may suffice. However it is important to have a low threshold for admission to hospital for IV antibiotics as cellulitis may be fatal. It may be recurrent, particularly in those patients with underlying lymphoedema or venous hypertension, and long term low dose antibiotic prophylaxis should be considered in high risk individuals.
Clinical Tip: Note that cellulitis is unilateral! It is VERY rare to see it bilaterally. Junior casualty officers often refer 'bilateral cellulitis' when in fact the diagnosis is usually varicose eczema with venous hypertension, allergic contact dermatitis to bandages or lipodermatosclerosis.

Cellulitis – hot, red leg. Note blistering also.

Post-operative cellulitis – note the marking to indicate if improvement occurring

Erysipelas of ear

Erysipelas- note the typical initial location under eye and at bridge of nose with significant oedema
Dissecting Cellulitis of the Scalp is really rather a misnomer as it is not a cellulitis! it is a condition seen young to middle-aged men with skin type 6 and consists of painless, deep, firm nodules, over the scalp. There may be marked bogginess and sinus tracts. Treatment is difficult but oral tetracyclines or intralesional corticosteroids. It is discussed in more detail in the module on Hair Disorders. I include it here for completeness.

Folliculitis and Boils
Folliculitis, by definition, is an inflammation centered around and of the hair follicle. Clinically one sees folliculocentric itchy or tender papulopustules, often with a central hair protruding from them. Superficial infection - usually staphylococcus aureus - produces the clinical appearance of folliculitis, whereas more deep seated infection results in boils or carbuncles (large boils).

Folliculitis - note visible hair emerging from folliculocentric pustule

Pseudofolliculitis is the term used for a folliculitis due to ingrowing hairs rather than true primary bacterial infection (e.g. shaving rash of beard area or shaved/waxed legs). The main problem here is inflammation due to the irritation of the hairs rather than primary bacterial infection. However the two conditions overlap in practice. "Sycosis barbae" is yet another term - implying an infected shaving rash, but again hair irritation plays a role as well. Advising the patient to leave a small length of beard and to use clippers rather than an electric razor may help. I sometime suggest topical anti fungal/weak steroid combination once week after shaving to help keep it at bay.

Sycosis barbae-commoner in skin type 6
There are lots of causes of folliculitis and indeed the cause may be multi-factorial - infection, shaving practices, racial (genetic) variation, climate/humidity, occlusive clothes, occlusive medical dressings, use of very greasy moisturisers, rich ointments or hair pomades.
There are a number of specific 'folliculitis' entities which are worth knowing about - some more common than others.
1. Hot-tub folliculitis -Unhygienic jacuzzis can be a source of infection which is due to pseudomonas. This often spontaneously resolves but can be treated with topical antibiotic if needed.

'Hot-tub'pseudomonas folliculitis. Note cut off at waist with lesions only in immersed areas.
2. Pityrosporum folliculitis on trunk (see below in 'fungal' section). Note very monomorphic lesions.

Pityrosporum folliculits. Often seen in athletes or those who work in hot, sweaty environments
3. "Steroid acne" is a folliculitis secondary to systemic steroids (it is not a true acne but rather is an acneiform eruption).

Steroid acne- associated with use of oral steroids. Note how monomorphic the lesions are in this typical location for this diagnosis.
4. "Itchy folliculitis" is a very itchy folliculocentric eruption seen on the upper trunk and limbs, secondary to HIV infection (cause unknown). It has many eosinophils histologically and usually responds to Tetracyclines, but it is important to know about it as it can be a presenting sign of HIV infection. It has sometimes been called 'eosinophilic folliculitis'.

5. Folliculitis (or acne) keloidalis – This is very common in young black adult males. It is a 'folliculitis' on the nape of neck and occipital scalp which can progress to hypertrophic scars or keloid with hair loss. Occasionally the condition is very severe with deeper infection – the whole occipital scalp is boggy and discharging with scarring alopecia (called "dissecting cellulitis of scalp" or "perifolliculitis capitis"). Treatment is very difficult. Try avoiding shaving and long-term (more than 6 months) oral antibiotics. For severe cases triamcinolone injection into the scarred area or radical surgery is indicated. It is not really a true folliculitis in the bacterial sense but is included here for completeness.

Treatment of folliculitis:
"Infective form" is with topical antiseptics, topical antibiotics (e.g. fusidic acid) or oral antibiotics (e.g. flucloxacillin 500mg or erythromycin 500mg both four times daily for 2-4 weeks or longer). Remember to think about itchy folliculitis in widespread chest folliculitis and whether any element of occlusion with grease or ointments is provoking the problem. Advise patients to avoid tight clothes, occlusive dressings, use lighter moisturisers, and to rub moisturisers in the direction of hair growth etc.
"In-growing hair form" - avoid shaving if possible or shave less closely, without stretching the skin. I often use a weak hydrocortisone-fungal combination after shaving as a precautionary measure and many patients find this helpful.
Hidradenitis suppurativa
I have included this condition under BOILS, although it is not a true staphylococcal/streptococcal infectious boil as such, but rather an inflammatory one which may be part of the so-called Follicular Occlusion Tetrad of conditions- Hidradenitis, Dissecting Cellulitis, Acne Conglobata and Pilonidal sinus. I have put it here though as patients usually present with what they describe as 'recurrent boils', and it is an important condition to be aware of. Fortunately it is a relatively rare condition but one which causes a vast amount of suffering to the patient.
It is characterised by a painful, discharging, chronic inflammation of the skin at sites rich in apocrine glands (axillae, groins, natal cleft). Patients tend to be females usually, but not always, with a high BMI and within some families it appears to be inherited in an autosomal dominant fashion. It presents after puberty with paired comedones, papules, nodules and abscesses which often progress to cysts and sinus formation. Lesions are in the axillae, groin, natal cleft and buttocks. Complications include fistulae, keloid scars, lymphoedema and contractures. The condition follows a chronic relapsing remitting course and aggravated by obesity, smoking and certain drugs e.g. Lithium. It is thought to be multifactorial - hormones, infection, apocrine gland structure and genetic predisposition (PSENEN & NCSTN genes).
Treatment is very difficult, particularly in moderate and severe disease and involves lifestyle measures such as stop smoking, lose weight, topical antispetics e.g. Chlorhexidine as soap. Mild disease can be managed with topical antibiotics such as Erythromycin and Clindamycin, along with staph elimination and bleach baths.
There are a number of therapeutic options for more severe disease which can often be very difficult to control, and include oral antibiotics: Tetracyclines, Clindamycin +/- Rifampicin, oral antiandrogens, isotretinoin/acitretin and in very severe cases biologic therapy with Infliximab. Surgery may be indicated. There is some suggestion that oral zinc sulphate 10mg/kg max 400-600 mg daily may be helpful in Hidradenitis, and a number of case reports using axillary Botox have suggested that this may be of benefit also.

Hidradenitis- typical locations and note typical bridging scarring in axilla.
Echthyma
This is an infection due to streptococcus or staphylococcus aureus or occasionally both which is rare in the UK but seen more commonly in debilitated, intravenous drug abusers immunosuppressed people (e.g. HIV), diabetics, the homeless alcoholics etc. It is more common in developing countries, being associated with poor nutrition and hygiene. Typically, chronic well demarcated, round, ulcerative lesions sometimes with an exudative crust are seen usually on the lower legs. Eschar like appearances can be noted and associated ulceration can be deep. It can usually be treated with oral antibiotics but remember if you do encounter a case to look for an underlying cause.

Echthyma – note the deep, black, crusted ulcers
Three 'Often Missed ' streptococcal diagnoses .
Perianal streptococcal cellulitis - quite common in children under age 10. Presents with perianal redness and soreness that may make defaecation painful. No systemic upset. Check skin swab for Streptococcus pyogenes. Responds to oral penicillin.

Streptococcal vulvo-vaginitis – usually caused by Strep. pyogenes presents as vulvo-vaginitis in pre-pubertal girls. Presents with genital soreness, dysuria and sometimes purulent discharge. Treatment - oral penicillin. Both the above can rarely occur in adults.

Blistering distal dactylitis - A large blister/pustule on tip of a finger (palmar) esp in children/young adults - swab it - responds to oral penicillin.

Toxin mediated Staphylococcal and Streptococcal diseases.
The conditions which we have just seen and discussed are all due to direct invasion of the tissue by the bacterium. Both staphylococci and streptococci can cause pathology by toxins and we will have a look at these here. Although this is not discussed further at this stage in the course, remember too that Streptococcal throat infection may cause exacerbation of psoriasis by antigen cross linkage in the skin.
Staphylococcal Scalded Skin Syndrome (SSSS)
Staphylococcal scalded skin syndrome (SSSS) is the most common of the toxin mediated disorders but even so, is fortunately rare. It presents as an acute toxic illness in children and is exceptionally rare in adults. The skin becomes bright red with superficial blisters and shedding (like a scald).
Clinical Tip - often starting in flexures and body folds with peeling skin.
Systemic upset with fever is usual and unlike toxic epidermal necrolysis (which it can mimic) there is no mucosal involvement. Staph aureus produces a toxin which attacks the outer part of epidermis, causing the typical peeling.

Staphylococcal scalded skin syndrome – unwell child, with red, peeling skin, initially flexural involvement
Prognosis is very good if treated with antibiotics (flucloxacillin). Remember that only the outer epidermis is damaged. The inner epidermis is preserved which preserves most of skin function (unlike in Toxic epidermal necrolysis where one sees full thickness epidermal necrosis). Patients should be seen by a dermatologist as an emergency.
Toxic shock syndrome
This is best known for occurring in tampon users. It is luckily fairly rare but can be fatal. Fever and an initial faint macular erythema or scarlatiniform rash is typical in the beginning, with mucosal erythema a common sign. 1-3 weeks later circulatory shock and multi-system disease occurs. Treatment involves antibiotics and supportive care.
Clinical Tip: Shocked female patients -ask if they are menstruating and using tampons.
Panton-Valentine leukocidin (PVL) associated disease and MRSA
PVL is a pore-forming toxin produced by several strains of staph aureus including community-acquired methicillin-resistant staph aureus. It is associated with recurrent necrotic skin and soft-tissue infections. Risk factors include compromised skin integrity; skin-to-skin contact with infected individuals and sharing of contaminated towels. It is common in students sharing accommodation and in individuals such as wrestlers or those indulging in contact sports. I recently saw a case of beard furunculosis due to PVL staphs in a professional cage-fighter. Infection of the hair follicle is the most common PVL-associated disease and usually presents as a large skin abscess, boils or furuncles with surrounding erythema. The lesions are often multiple and are often associated with systemic upset, e.g. fever. You need to specifically request PVL testing on the swab if you are suspicious of PVL, as labs won't routinely do it.
The treatment of choice is surgical drainage of the abscess but if antibiotics are needed, Clindamycin, Linezolid and Rifampicin can be used although specialist microbiology advice should be sought in these cases.
Clinical Tip: Occurs in students, contact sports, deep abscesses
One of the reasons why PVL staphs are important to recognise is that it can cause widespread septicaemia and pulmonary infection and fatalities have been reported.
Clinical Tip: Get patients to stop smoking if they have had MRSA/PVL infections
Clinical Tip: MRSA /PVL patients and their families should be advised to decolonise their living environments by using alcohol wipes/gel to toilet handles/computer keyboards/fridge doors etc and decontaminate pets

PVL staph abscesses in a teenage patient
Streptococcal toxic shock syndrome is very similar to the above, associated with invasive Group A Strep (throat, wounds, soft-tissue).
Scarlet fever is caused by Strep pyogenes (a Group A strep) usually from a sore-throat, which produces a toxin. There is fever, then 1-2 days later, punctate erythema progressing to erythroderma (mild purpura in skin creases and perioral sparing is characteristic). Mucosal erythema is common. By day 7-10 skin shedding occurs. It can occasionally be very severe and coma and myocarditits have been reported. Complications also include suppurative: arthritis, meningitis, and osteomyelitis. Fortunately it is much less common than in the last century and also less severe. Treatment - penicillin and supportive care.

Scarlet fever
Meningococcal disease
Although this is not a skin disease as such, the presence of purpura on the skin is such an important clinical sign not to be missed that I feel duty bound to include it in this chapter. Remember your patient may be feverish, have a headache and photophobia but they may not look unduly unwell at the beginning so LOOK AT THE SKIN very carefully all over.
Clinical Tip: Meningococcal purpura, unlike a leucocytoclastic vasculitis which tend to favour the lower legs, can occur anywhere on the body, with non blanching often irregularly shaped purpuric or dusky skin changes.

Meningococcal sepsis- note non blanching irregularly shaped purpura
Invasive Infections
Thank goodness these are rare but I have included them here as they are very often fatal and again it is imperative not to miss them.
- Necrotising fasciitis This occurs most commonly in elderly, debilitated and diabetic especially post-surgery. It may be streptococcal or due to mixed infection. The patient may not be toxic in the early stages but the most striking finding is of severe pain, often seeming to be out of proportion to what one sees on the skin surface. Tender erythematous skin evolves into a rapidly spreading area of black necrosis around the wound. Treatment is with immediate extensive surgical debridement, antibiotics and supportive care.

- "Fournier's gangrene" is a version of the above that often starts in the scrotum/lower abdomen.

Infections caused by Corynebacterium
Corynebacterium (the bug also responsible for Diphtheria) can cause 2 rashes:
Erythrasma
Presents as an orangy-brown flexural rash often seen in the axillae or toe web spaces. It is frequently misdiagnosed as a fungal infection but the very distinct colour is usually helpful in making the diagnosis. The rash shows a dramatic coral pink fluorescence under Wood's (ultraviolet) light. It is caused by Corynebacterium minutissimum and is easily treated with Erythromycin either orally or I often use the topical form which is licensed for use in acne. -oral Erythromycin (500mg four times daily for 10 days).

Erythrasma – orangy-brown rash in groin Fluoresces pink under Wood’s light
Pitted keratolysis
This is a superficial infection of the horny layer of the skin frequently involves the soles of the forefoot and appears as numerous small punched-out circular lesions of a rather macerated skin (e.g. as seen after prolonged immersion). There is usually an associated hyperhidrosis of the feet and a prominent odour. It can be confused with mosaic warts but when you look carefully you will see that there are pits rather than black dots (which are seen in warts).
Treatment: topical antibiotics (e.g. fusidic acid, clindamycin or erythromycin; apply twice daily for 2-4 weeks) and topical anti-sweating lotions.

Pitted keratolysis - clustered white punched-out pits
VIRAL INFECTIONS
Viruses can cause many different appearances on the skin! Rashes or lesions caused by viruses may be -
- Macular
- Maculopapular
- Vesicular
- Purpuric
- Warty
1. Vesicular rashes
Typically rashes with vesicles tend to be caused by one of the following.
- Herpes simplex
- Varicella zoster
- Poxviruses
- Coxsackie virus
- Entero/echo viruses
Herpes zoster and varicella zoster
Varicella is the term used to describe classical ‘chickenpox’. The incubation period is 21 days and there may be an influenza – like prodrome prior to the rash. The rash classically starts centrally and then spreads, particularly to areas not exposed to pressure e.g. axillae; it is rare on the palms or soles. Lesions appear in crops, initially appearing as macules and then developing into papules, which become vesicular and then crust as the vesicles burst. There are usually lesions at all stages visible. Recovery from infection gives lifelong immunity. The virus remains latent in one or more posterior root ganglia. Remember infection may be more severe in adults, in immunocompromised and in smokers who are at risk of developing Chicken pox pneumonitis.
Clinical Tip: Look in Axillae (often involved) and look for lesion 'Dew Drop on a Rose Petal'- vesicle on erythematous base

Varicella – note lesions at different stages in development

Dew Drop on Rose Petal
Herpes zoster refers to the reactivation of varicella zoster virus causing a unilateral rash in a single dermatome (shingles), most commonly the ophthalmic branch of the trigeminal nerve and on the trunk in the distribution of T5-L2. The rash may be preceded by an area of paraesthesia and hyperaesthesia where the rash develops and with weakness in the affected or adjoining limb. The rash is also vesicular and heals with crusting. The majority of cases occur over the age of 50 years.
Clinical Tip: Asking about preceeding dysaesthesia in the skin is a really helpful way to aid making the diagnosis, particularly if you are not sure.

Herpes zoster – note the dermatomal distribution
What if the rash is not confined to one dermatome? How can you determine whether the infection is primary or a reactivation (shingles)?
This is initially determined from the history. Questions to ask:
- Is there a history of chickenpox
- Has there been any contact with chickenpox? Patients are infectious from 24-48 hours prior to the rash and until all vesicles have crusted, usually 5-7 days. Spread occurs via respiratory droplets. In practice spread will only occur after a prolonged period of time in close proximity e.g. 15 mins face to face contact or 30 mins in the same room. Contact prior to 48 hours before the rash can be disregarded.
- What age is the patient? Zoster is more common in the elderly, but may occur in children with a history of varicella occurring in utero or in infancy. Healthy children presenting with shingles therefore may sometimes need to be investigated for causes of immunosuppression.
- Is the patient immunosuppressed? Very immunosuppressed patients e.g. those receiving chemotherapy, may occasionally present with ‘disseminated shingles’ i.e. several dermatomes affected. They will also be generally unwell with a fever and tachycardia and should be referred to hospital for intravenous Aciclovir.
Clinical Tip: Multi-dermatomal shingles can be a presenting sign of HIV infection and should ring alarm bells.
Laboratory diagnosis
1. Serology: is this primary or secondary? If it is unclear whether the patient has had varicella in the past a serum sample (clotted blood) should be sent to the lab for varicella IgG. If this is positive this indicates past infection and therefore immunity. Patients with zoster will have preexisting IgG antibody. Patients with chickenpox may be positive for VZV IgM antibodies but are often seronegative at presentation. If a blood sample is sent at the onset of the rash a repeat specimen should be sent after recovery to detect seroconversion (development of IgG).
2. Direct immunofluorescence: is this varicella? The simplest and fastest way of obtaining a diagnosis of varicella is by sending a scraping from the base of a vesicle on a slide to virology, and a swab from the base of the lesion in viral transport medium for culture.
Infection control and contacts
Anyone without a past history of varicella is at risk of developing the disease after exposure. The disease can be more serious in adults, particularly those who smoke, due to the risk of varicella pneumonitis. Immunosuppressed individuals and neonates are at increased risk of haemorrhagic or disseminated varicella. There is also an increased risk of varicella pneumonitis in pregnant women, along with the risk of congenital varicella syndrome in the foetus. Congenital varicella syndrome includes limb hypoplasia and skin scarring, microcephaly, cataracts and growth retardation. The risks to the foetus have been estimated to be less than 1% in the first 12 weeks pregnancy and approximately 2% between weeks 13 and 20. After this gestation maternal infection may cause herpes zoster in the infant, up to the week before and after delivery when infection can be severe or fatal in the infant.
First determine whether contact occurred in the infectious period (see above). Pregnant women whose immune status is unknown should have an urgent VZIgG assay requested (obtain advice from the lab). This can be done the same day by the lab if necessary. Human varicella zoster immunoglobulin (VZIG) is recommended as prophylaxis for individuals fulfilling all of the following three criteria.
(a) a clinical condition which increases the risk of severe varicella e.g. immunosuppression, pregnancy, neonates
(b) no antibodies to varicella
(c) significant exposure to chickenpox or herpes zoster
VZIG is obtained from the virology department and is only effective if given within 10 days of exposure, preferably within 72 hours. It does not prevent infection but may attenuate disease.
Healthcare workers without varicella antibodies should not have contact with patients during their incubation period, returning to work 21 days after exposure. Individuals who have received VZIG have longer incubation periods. Ideally the immune status of immunocompromised patients should have been checked and susceptible individuals should be immunised and advised to avoid contact with infected individuals.
Apart from the issue of timing of the contact, as described earlier, the type of contact and closeness and duration of contact are important. The need for VZIG is restricted to those in contact with chicken pox, disseminated zoster, immunocompetent individuals with exposed lesions (e.g. ophthalmic zoster) or immunosuppressed individuals with lesions anywhere (viral shedding may be greater). A significant duration of contact would be 30 mins or more within the same room, or face-to-face contact e.g. having a conversation. Transmission from household contacts is particularly efficient.
To obtain VZIG contact your local virology department for advice. It will either be issued from the department itself or from Public Health Laboratories and the Communicable Disease Surveillance Centre (CDSC).
In the UK varicella vaccine is available privately but the UK's immunisation body decided against universal vaccination of children. Patients not immune to chickenpox who are at risk of complications from varicella if they are exposed, may discuss vaccination. It may also be recommended for healthcare workers and close contacts of immunosuppressed who are not already immune. The vaccine is given as two separate injections, usually into the upper arm, four to eight weeks apart. The varicella vaccine is effective in making about 90% immune. The vaccination cannot be given in pregnancy and pregnancy should be avoided for 3 months after the injection.
Management of chicken pox
Children: it is a self-limiting illness and management is supportive. They should avoid pregnant women and immunosuppressed patients (but, not necessarily other children). Aspirin should not be given due to the risk of Reye’s syndrome, a syndrome of encephalopathy and liver damage associated with varicella and influenza. Topical antipruritics such as Calamine lotion are very old fashioned but do seem to afford relief from itch. A mild antihistamine may be advised.
Adults: treatment is also supportive, but they should be monitored for complications of varicella. Treatment with aciclovir is indicated for otherwise healthy adults presenting within 24 hours of the rash who smoke and/or have chronic lung disease and pregnant women in the second half of pregnancy. Treatment is also indicated in adults who develop respiratory symptoms and a fever (may require intravenous therapy therefore seek specialist advice- there is also a risk of permanent lung fibrosis).
• Secondary bacterial infection of skin
- Viral pneumonia occurs in 1 in 200 adults (compare with 1 in 200,000 children) 10% smokers increased risk in immunocompromised individuals and pregnancy.
- Haemorrhagic chicken pox. Lesions may appear purpuric. May be associated with thrombocytopenia and disseminated intravascular coagulation so seek specialist advice.
- Encephalitis cerebellar ataxia in children- most recover fully but it may take months. More common in immunocompromised. 3-4/100,000 cases in children.
Management of Shingles
Early treatment with high dose acicilovir (800mg orally 5 times per day) has been shown to reduce zoster-associated pain, produce faster resolution of the rash and decrease eye complications. Oral famciclovir (dose 250mg three times tds) seems to be as effective. There is some evidence that low dose amitryptiline given early also helps reduce intensity and duration of pain. Prednisolone given acutely with aciclovir reduces acute symptoms but does not seem to shorten duration of zoster associated pain (ZAP). Sympathetic nerve blocks have been reported anecdotally to reduce ZAP. Mild opiate analgesics will provide relief during the acute attack. Furthermore, gabapentin, a GABA analogue has been shown to reduce pain of three months duration. Carbamazepine should not be used- this is effective in trigeminal neuralgia, not herpetic neuralgia. Acupuncture may provide pain relief for some patients, along with topical measures such as ice packs and capsaicin. Patients with intractable pain may benefit from referral to a specialist pain clinic.
Primary herpes simplex infection
Clinical Tip: With Herpes Infections look for lesions in groups/clusters. Lesions are monomorphic usually (unless secondarily infected).
Primary herpes infections can cause
- Gingivostomatitis: infection may involve the buccal and gingival mucosa, tongue and fauces. Vesicles evolve into shallow painful ulcers on an erythematous base; they may coalesce if extensive. Other features include fever, submandibular lymphadenopathy, febrile convulsions in children and abnormal liver function tests. The lymphadenopathy may persist for several weeks after the ulcers have healed. Conjunctivitis, myalgia, abdominal discomfort and pharyngitis may also occur. Oral disease may be associated with lesions elsewhere, possibly caused by autoinoculation from the site of primary infection. The incubation period is 2-12 days and illness duration is usually 2-3 weeks.

Note clustered monomorphic lesions
- Genital infection: the lesions are located principally on the vulva in women and may extend to the perineum, upper thighs and buttocks. In men, vesicular lesions are seen on the glans penis or penile shaft. Secondary bacterial infections may occur, requiring antibiotic therapy. Sacral radiculitis, associated with urinary retention and neuralgia may occur. Primary genital infection is associated with fever, dysuria, urethritis, inguinal lymphadenopathy and malaise, and lasts up to 3 weeks. Recurrent genital herpes may occur with more scanty vesicular lesions associated with localised irritation rather than significant pain. New vesicles may occur after the initial lesions have crusted over, delaying healing. Complications are rare with recurrent infection.

Clinical Tip; Complex, multi-site or slow to resolve perianal or gential HSV should alert you to the possibility of underlying HIV infection
- Eczema herpeticum/ kaposi’s varicelliform eruption: a superinfection of eczematous skin, especially in young children. There are usually systemic symptoms such as fever and lymphadenopathy. As these patients are often on steroid treatment this facilitates the spread of the virus, and untreated this condition has a significant fatality rate. Patients should be advised to take care with close contact with relatives with coldsores.
Clinical Tip- Look for groups of monomorphic punched out lesions. Don't expect to see intact blisters.
- Herpetic whitlow: an inflammation at the nail fold due to direct inoculation of the virus into the fingers through a portal of infection. This is common in health care workers especially those involved with manipulation in the mouth (e.g. anaesthetists, dentists), but may also been in nail biters and workers such as laboratory personnel who sustain a traumatic injury with contaminated needles or glassware. The whitlow is extremely painful and takes about four weeks to heal.

Herpetic whitlow. Can be differentiated from dactylitis by the presence of grouped clustered vesicles
- Conjunctivitis and keratitis: both the conjunctiva and cornea may be involved and there may be visible vesicles and ulcers on the eyelids.
- Erythema multiforme (EM). Mycoplasma pneumonia and HSV are the infectious agents most commonly recognised as precipitants of EM. Erythema multiforme does not respond to aciclovir but recurrent cases can be prevented by prophylactic acyclovir. Sometime in more severe EM it may be necessary to treat with oral steroids.

Erythema multiforme- typical acrally distributed targetoid lesions

Typical cold sore of HSV1

Vesicles in Herpes simplex infection- note the typical clustering
HSV in the immunocompromised
Infection begins usually in either the oral or genital sites and can progress rapidly to extensive ulceration. Cutaneous dissemination may make the rash look like varicella. There is also a risk of visceral dissemination causing encephalitis, pneumonia and hepatitis. In patients with HIV recurrent infection may occur at multiple sites with high frequency and the lesions may be slow to resolve.
The virus establishes a latent infection of dorsal root ganglia, the trigeminal ganglia for HSV-1 and the sacral ganglia for HSV-2. Reactivation of the virus produces recurrent infection. The triggering process is not understood but a variety of stimuli have been implicated: common cold, sunlight/ ultraviolet light exposure, stress, menstruation, infection and mild trauma. Severe primary infections are associated with a higher frequency of reactivation.
As for varicella zoster, the simplest method to make a diagnosis is to send a scraping from the base of a vesicle on a slide to virology, and a swab from the base of the lesion in viral transport medium for culture. Type specific varicella antibody detection is not generally useful, but may be performed in special cases after discussion with the virology lab e.g. repeatedly culture negative lesions which appear clinically to be HSV.
Primary HSV1 is often mild and symptomatic treatment may be all that is needed e.g. chlorhexidine mouthwashes and simple analgesia in the case of gingivostomatitis. Primary HSV2 infection may be more severe and is more likely to present with fever. In severe cases oral aciclovir, valaciclovir or famciclovir is recommended. Steroid treatment should be withheld or reduced as it increases the severity of the disease, although as mentioned earlier it is sometimes used in more widespread EM. Aciclovir cream may be useful in the treatment of recurrent infection but the most effective treatment for severe recurrent infections is a 5-day course of oral acyclovir commenced when prodromal symptoms begin. Patients with frequent recurrences should be considered for continuous suppressive therapy.
Primary infection during the first and second trimester of pregnancy is not associated with a significant risk to the foetus. Most cases of neonatal herpes occur as a result of perinatal infection. Infection in the third trimester is associated with a risk of transmission to the baby during vaginal delivery and risk is highest when infection occurs around the time of delivery. The mothers of most infants who develop neonatal herpes do not have genital lesions at delivery. Primary genital herpes poses the greatest risk but there is also a risk with recurrent infection. A few cases occur due to transfer of the virus from oral lesions to the infant post delivery. Most cases are due to HSV-2, but HSV-1 can also cause neonatal herpes. Symptoms appear 4-5 days post partum, with evidence of skin, eye and mouth infection. The infant may also develop encephalitis and disseminated disease involving lung, liver, adrenals, eyes and skin. Mortality is greater than 80% for disseminated disease, without treatment. Most babies exhibiting only skin, eye and mouth involvement will develop permanent ocular damage and eventually show some evidence of neurological impairment. All HSV infections identified in the neonatal period should be treated with an antiviral agent. Caesarian section is recommended if clinically apparent cervical infection is present at parturition; delivery by either vaginal or Caesarian should be rapid to minimise exposure.
Other viral causes of vescicular rashes
• Coxsackie viruses can cause herpangina and hand, foot and mouth disease.
Herpangina is characterised by a painful eruption of vesicles in the mouth and throat, including the soft palate (unlike herpes simplex), fever and abdominal symptoms. It is commonest in children aged 2-10 years and is self limiting.
Hand, foot and mouth disease consists of an ulcerative exanthem of the buccal mucosa, mild fever followed by painful vesicular lesions on the hands or feet. It may spread within families and is also self limiting. Sometimes the lesions look more like a little paper cut on a base of erythema.

Vesicles on sole in Hand foot and mouth disease
• Parapoxviruses: can cause orf, a contagious pustular dermatitis contracted from sheep and goats, and paravaccinia (pseudocowpox, ring sores) which is contracted from cattle. Infection is localised and occurs via cuts and abrasions. Lesions start as erythematous papules and progress to a ‘target’ lesion 1-2 weeks after infection, appearing as a red centre surrounded by a white halo and an outer erythematous halo. The lesion then becomes nodular and then papillomatous, often with a weeping surface, and resolves over a period of weeks with crusting. Occasionally lesions become large and granulomatous, needing surgical removal. Vesicles are occasionally visible to the naked eye, but the lesion generally does not look classically vesicular. Most patients have a single lesion only, which is mildly painful. The patient is normally systemically well although lymphadenopathy and malaise may occur. Diagnosis is clinical, but samples of the lesion may be sent to the virology lab for detection of the virus using electron microscopy. Infection may spread between human contacts, so patients should be advised to avoid spreading the infection by contact with broken skin.

Maculopapular rashes may arise following infection with any of the following:
- Rubella
- Parvovirus
- Entero/Echovirus
- Measles
- EBV
- CMV
- Dengue
Viral causes of a maculopapular rash according to age group
| Age <1 year | 1-5 years | 5-10years | 10-15years | Adults |
| HHV6 | HHV6 | Parvovirus | EBV | Rubella |
| Rubella | Rubella | Rubella | CMV | Parvovirus |
| Measles | Measles | Rubella | ||
| Parvovirus |
Parvovirus infection 'Slapped cheek'
50% infections are asymptomatic. Otherwise there is commonly a biphasic illness consisting of a brief prodrome of a non-specific febrile illness with a cough, followed by recovery and approximately seven symptom free days. Then the classical fiery red, macular ‘slapped cheek’ rash develops which spares the area around the mouth (circumoral pallor) and has slightly raised edges. The rash spreads 1-4 days later to involve the trunk and limbs and becomes maculopapular, resolving with central clearing to form a lacy (reticular) pattern. It is most prominent on extensor surfaces and is itchy. It rarely affects the palms or the soles and can look very similar to rubella. It lasts 1-3 weeks and fluctuates with environmental factors e.g. it may flare after a hot bath.
Caused by Parvovirus B19 it is spread by droplets. It is usually benign but may cause the following problems:
- Joint involvement is rare in children but common in adult females (80% infections with a rash). In this group joint arthritis may occur without a rash, and is commonly a sudden onset symmetrical arthritis affecting the small joints of the hand, usually the proximal interphalangeal joints (PIPs). The arthritis usually resolves within 4 months.
- Aplastic crises may occur in patients with chronic haemolytic anaemia e.g. sickle cell disease. There is a sudden fall in haemoglobin which may last 5-7 days due to a lack of red cell precursors (reticulocyte count will be low). The patient will present with symptoms of anaemia.
- Chronic anaemia may occur in immunocompromised patients who have failed to produce neutralising antibodies and have chronic parvovirus infection. The anaemia resolves after administration of Normal Human Immunoglobulin (NHIG) and these patients may develop a rash illness subsequently, due to the deposition of immune complexes.
- There is no evidence that parvovirus causes birth defects. However, foetal hydrops may occur due to 2nd or 3rd trimester infection and may occur from 2-12 weeks after the rash. For this reason women who have had parvovirus infection in pregnancy should be monitored closely to assess the development of hydrops in the foetus. Such babies may require foetal exchange transfusions. Termination is not advised if there is no evidence of hydrops and the pregnancy is proceeding normally but specialist advice should be sought. Miscarriage has been reported in the first trimester following contact with B19.
Diagnosis is usually clinical but if necessary a clotted blood sample can be sent for the detection of parvovirus specific IgM (indicating current infection) and IgG (indicating previous/current infection). Ideally a blood sample should also be sent from the index case to confirm parvovirus infection. In the case of immunocompromised patients the virus can be detected using PCR to detect viral DNA in the serum.
B19 can also cause the Purpuric Glove and Stocking eruption in adults.

Slapped cheek
Rubella
Infection may be asymptomatic in up to 25%. Adults may experience prodromal symptoms of malaise and fever for a day or two before the rash but in children the onset is usually abrupt, with the appearance of the rash. The rash starts on the face as macular lesions and then spreads to the trunk and limbs. It seldom lasts for more than 3 days and may also be seen on the soft palate. There is usually pharyngitis and enlargement of the cervical, and especially the suboccipital and postauricular lymph nodes. Lymphadenopathy may be generalised and tender, may present up to a week before the rash and persist for 10-14 days after the rash. Constitutional symptoms are usually mild in children. N.B. the rash is not diagnostic of rubella as other viruses may cause the symptoms.
Clinical tip: the rash is often a very specific 'pillar box' red in colour and look for occipital lymph nodes.
It is usually benign but the following complications are recognised
- Arthralgia- rare in children but may occur in up to 50% of adult females. It usually develops as the rash subsides and persists for less than a week (occasionally longer). The most common joints affected are the finger joints, wrists, knees and ankles. The arthralgia is believed to be mediated by immune complexes but hormonal factors may play a role because in female vaccinees joint symptoms are most likely to develop within 7 days of the onset of the menstrual cycle.
- Postinfectious encephalomyelitis may develop in 1 in 5000-10,000 cases within a week of onset of the rash. It is not associated with demyelination or inflammatory damage and the prognosis is good.
- Thrombocytopenic purpura is rare.
- Primary maternal rubella infection in the first ten weeks of pregnancy results in foetal damage in up to 90% of infants. The risk of damage declines to 10-20% by 16 weeks and is rare after 16 weeks. Congenital rubella syndrome consists most commonly of a triad of cardiac abnormalities (e.g. patent ductus arteriosus, ventricular septal defect), cataracts and deafness. Other abnormalities include mental retardation, growth retardation, hepatosplenomegaly, jaundice, anaemia, thrombocytopaenic purpura and bony lesions. Any combination of defects may occur, although perceptive deafness and pigmentary retinopathy may occur alone. Infants may appear normal at birth. Rubella re-infection has a lower risk of foetal infection, approximately 8% in the first 16 weeks of pregnancy, and foetal malformations are rare. Infants with congenital rubella syndrome are highly infectious, excreting virus from their pharynx and in urine. Approximately one third will still excrete virus at 6 months of age, although this seems to be rare after the age of 2 years.

There is good immunity after both naturally acquired rubella and vaccination. However, reinfection may occur and can be asymptomatic. It is diagnosed by demonstrating a significant rise in specific anti-rubella IgG following exposure.
All pregnant women with possible rubella infection or exposure to rubella need to be investigated serologically regardless of a history of previous rubella or vaccination. Blood should be taken as soon as possible after the onset of symptoms or exposure to detect the presence of rubella specific IgG and IgM. No particular titre of antibody is indicative of present or recent infection-a further sample should be sent 7-10 days later to detect a significant rise in antibody titres. Low levels of IgM may be detected for up to 4 years following rubella vaccination and may be detected in reinfection so this result is not diagnostic of recent primary infection. A good clinical history of LMP, timing of exposure, symptoms and previous infection/ vaccination will help in the interpretation of the results. Sending a blood sample for detection of rubella IgM or a salivary swab if the case is a child should do confirmation of rubella in the index case.
The vaccine consists of live attenuated virus and is therefore not recommended in pregnancy. Susceptible women should be vaccinated after delivery. Pregnancy should be avoided for one month after rubella vaccination.
Post exposure prophylaxis with HNIG is of little value as it does not prevent infection in non-immune contacts, although it may reduce the likelihood of clinical symptoms. Its only recommended use is for when termination for confirmed rubella would be unacceptable, and it should be given soon after exposure.
Other viruses which cause rubelliform rashes and arthralgia
Parvovirus B19, enteroviruses (coxsackie A, echovirus) and some arboviruses e.g. Ross River virus.
Measles
Prodromal symptoms are respiratory and usually consist of fever, malaise, rhinitis, conjunctivitis and cough. The patient is highly infectious at this stage. Koplik’s spots may appear on the buccal mucosa inside the cheek and mouth; these tend to fade as the rash begins. The main illness consists of fever and a dusky red maculopapular rash which starts on the forehead and behind the ears and spreads to the rest of the body. It fades to a brownish colour and resolves with fine desquamation. It is not itchy. Generally, the fever, conjunctivitis and respiratory symptoms subside when the rash is at its peak.
The incubation period is approximately 10 days, the prodrome lasts 2-4 days and the rash appears approximately 2 weeks post exposure. Spread is via the respiratory route. Patients are infectious from the beginning of the prodrome until four days after the appearance of the rash. The incidence increases in winter and early spring.

Kopliks spots in buccal mucosa
Complications of measles
- Opportunistic infections can occur, particularly bronchopneumonia, croup and otitis media.
- Giant cell pneumonia: rare, usually only in immunodeficient or with chronic debilitating disease. It is caused directly by measles virus and is very severe.
- Measles inclusion body encephalitis: only in immunosuppressed, presents with convulsions, myoclonic jerks, coma and stupor. Death occurs within weeks or months; the course is more rapid than subacute sclerosing panencephalitis (SSPE).
- Acute measles postinfectious encephalitis: occurs in 1 in 1000-5000 cases of acute measles and 20-40% have lasting neurological sequelae such as fits, hemiplegia and mental retardation. It develops with fever, headache, seizures, cerebellar ataxia and coma. The mortality rate is 15%.
- Subacute sclerosing panencephalitis (SSPE): usually occurs in children and young adults 6-8 years after acute measles and has an incidence 1 per million cases. It is commonest in children who had measles before the age of 2 years. The illness lasts 13 years and leads to death. It is characterised by generalised intellectual and psychological deterioration, fits, aphasia, myoclonic jerks and chorioretinitis. There are characteristic EEG changes. It is due to persistent measles infection and patients have high titres of anti-measles IgG and IgM in serum and CSF.
- Other complications include hepatitis, myocarditis, pericarditis and mesenteric lymphadenitis.
- Case fatality rates for measles are age related- high under the age of 1year, lowest for the age group 1-9 years, then increasing with age.
A saliva sample should be sent for specific measles IgM, ideally 3 days after the onset of the rash. A blood sample may be sent at the time of diagnosis, for the detection of measles specific IgM, followed by a further sample 7-10 days later to detect a rise in antibody titre.
Contact with measles poses a risk for children under the age of 1 year, the immunocompromised, and those with chronic debilitating disease. Parents who do not remember either having measles or being vaccinated are also at risk. It is therefore of importance that these individuals be immunised. Susceptible individuals at risk may be protected after exposure by the administration of human normal immunoglobulin, given within 3 days of exposure. Effectiveness disappears if given greater than 6 days after exposure.
The illness is normally self-limiting, but complications such as bacterial infection will need to be treated with antibiotics. More severe complications will obviously necessitate referral to hospital.
Roseola infantum
Caused by Human Herpes Virus 6 (HHV6)
Primary HHV6 infection usually manifests in children as an acute febrile illness lasting 3-4 days; 10% will also have a macular or papular rash on the face and trunk similar to measles or rubella (it is commonly misdiagnosed). Transmission is via salivary secretions. Complications include febrile seizures, hepatitis, bone marrow suppression, encephalitis, gastrointestinal symptoms and respiratory symptoms (pneumonitis in 10%). HHV6 infection accounts for a third of febrile seizures under the age of 3 years.
The diagnosis is generally clinical, but in some circumstances (e.g. child with neurological complications) indirect immunofluoresence and PCR can be used to identify the virus. These investigations are generally done by a reference lab and need to be discussed in advance.
Other main causative agents of a maculopapular rash
Both Epstein-Barr virus (EBV) and Cytomegalovirus (CMV) can cause infectious mononucleosis. The seropositivity of EBV increases with age, with greater than 90% of adults worldwide being seropositive: conversely, primary EBV is unusual in the middle aged and elderly. There are two age groups in whom infection peaks; 1-6 years and 14-20 years.
EBV infection
It may be subclinical in healthy adults (50% infections) or present abruptly with a painful throat, fever, malaise, headaches, neck stiffness, anorexia and vague abdominal discomfort. Palatal petechiae occur in the first week of illness, and they may be associated with a greyish membrane and exudative tonsillitis. Two types of rashes are seen; a generalised, faint, non-itchy morbilliform rash lasting under 2 days, and a florid maculopapular rash seen in patients given penicillin. Generalised lymphadenopathy occurs, the nodes being palpable for several weeks. Splenic enlargement occurs in 50% patients and hepatomegaly, mild jaundice and derangement of liver function also occurs in a significant proportion of cases.
Close contact: the virus is present in salivary secretions. The incubation period is 30-50 days.
Complications
- Pharyngeal oedema and tonsillar enlargement can result in obstruction of the pharynx or trachea.
- Splenic rupture is very rare.
- Neurological complications such as meningitis, encephalitis or Guillain-Barre syndrome may precede, accompany or post-date Infectious mononucleosis by weeks.
- Hepatic complications: jaundice occurs in 5-10%.
- Chronic cases can occur where symptoms persist for greater than 1 year (approx 1 in 2000) cases. The average duration of symptoms is 2-3 weeks.
- Immunological complications include haemolytic or aplastic anaemia, thrombocytopaenia, agranulocytosis and hypogammaglobulinaemia.
Clinical Tip: Affected individuals should be warned to avoid contact sports for at least 6 months following infection if their LFTS are abnormal due to the risk of splenic rupture if kicked etc.
Diagnosis is made by full history and in the interpretation of any investigations
- Blood film: the presence of atypical lymphocytes is highly suggestive, although they are also seen in CMV infection, hepatitis B, influenza B and rubella.
- Monospot: detects IgM heterophile antibodies which cause haemagglutination of erythrocytes from species other than humans (sheep are usually used).
- EBV VCA IgM (viral capsid antigen): demonstration of IgM antibodies is diagnostic of recent infection. Demonstration of IgG antibodies is not usually helpful as they are usually present in the first serum sample taken after diagnosis.
Treatment is supportive; analgesia for the painful throat and paracetamol for fevers. Obviously penicillin should be avoided.
Pityriasis Rosea and HHV6/HHV7
There is increasing evidence that Pityriasis Rosea is associated with HHV6 and 7 infection. It most commonly affects ages 15-30 and starts with the typical 'herald patch' usually the trunk. The hallmark is the erythematous macule with peripheral collarette scale which follows on the trunk, often following the lines of the ribs (the so-called Christmas Tree distribution). This is best seen if you stand a little way back from the patient and observe the back of the chest from a slight distance. Rash may be a little itchy but usually asymptomatic. My old boss used to tell me it lasted Forty days and Forty nights!!
It doesn't usually need treatment although a mid strength topical steroid may relieve lesions and very rarely I prescribe narrow band UVB for protracted cases. Occasionally an inverse pattern can occur.
Clinical Tip: Look for Christmas Tree pattern and be aware that secondary syphilis may mimic Pityriasis rosea.


Pityriasis rosea- note typical Herald Patch and Christmas tree distribution following ribs
Cytomegalovirus (CMV)
Clinical presentation is similar to above but the majority of cases in otherwise healthy adults are asymptomatic.
Incubation is 4-8 weeks for a primary infection. Transmission can occur via saliva, sexually (particularly homosexual men) and more rarely from blood transfusion or organ transplantation. It is also transmitted perinatally via swallowed genital secretions and breast milk, and can occur as a congenital infection.
Primary CMV infection in the first 28 weeks of pregnancy causes a risk of cytomegalic inclusion disease in the foetus of about 4%. However, the presence of intrauterine infection does not necessarily cause clinically evident disease in the infant, the majority of these infants developing normally. These cases are difficult and should be discussed with the virologist and obstetrician. Ultrasound scanning and amniotic fluid testing for CMV may help identify potentially damaged cases. In the case of pregnant healthcare workers exposed to infectious CMV cases there is little evidence that they have an increased risk of developing infection, but good hygienic measures should be advised.
Symptomatic infants are described as having the syndrome of ‘cytomegalic inclusion disease’ which includes intrauterine growth retardation, jaundice, hepatosplenomegaly, thrombocytopenia, encephalitis, microcephaly, pneumonitis, myocarditis, hepatitis and congenital abnormalities of the 1st branchial arch and anophthalmia. Of those infected, 7% will be symptomatic at birth and 1% will die in infancy. Those which survive suffer fits, spastic diplegia, perceptual organ damage such as optic atrophy and deafness, and mental retardation. Of those infants which are asymptomatic at birth 15% will have hearing defects and/or mental retardation. Congenitally infected infants excrete CMV in urine, saliva and nasal secretions and so care should be taken to avoid close contact with pregnant women.
Diagnosis
The virus can be isolated from urine samples and saliva soaked into a cotton tipped swab sent in viral transport medium. Virus can be more rapidly detected in urine using the DEAFF test. The presence of CMV IGM in an acute blood sample is diagnostic of recent infection. PCR of plasma, whole blood and lymphocytes can be used to diagnose systemic viraemia. This is useful in monitoring immunosuppressed patients on therapy.
Again, management is supportive. Antiviral therapy is only indicated for serious or life-threatening CMV infection in the immunocompromised.
- Coxsackie A and echovirus can cause a fine rubella-like rash. It may be associated with fever, malaise and cervical lymphadenopathy and recovery is usually uneventful.
- Dengue virus often causes a diffuse, discrete maculopapular rash, heralding the recovery phase of dengue fever.
WARTS
These are predominantly caused by -
- Poxviruses
- Papilloma viruses
Warts are caused by Human Papilloma viruses (HPV) which infect and replicate in squamous epithelium. They enter the skin through small abrasions. The incubation period is probably a matter of months.
Common warts: firm papules with a rough horny surface. They are commonest over the knuckles and nail folds, and can also occur on the knees and on the shaft of the penis. They are caused by HPV 1, 2 and 4.

Common warts on fingers
- Plantar warts (verrucae) generally occur at pressure points. They start as a small papule and as they enlarge small thrombosed capillaries may be seen in the tips of the elongated papillae.
- Plane warts: smooth, flat or slightly elevated, occurring on the face or the back of the hands. They may form lesions at the site of abrasions (Koebner’s phenomenon). They are caused by HPV 3 and 5.

Plane warts
- Filiform warts are common in the beard area, on the lips and in the nasal vestibule.

Filiform wart
- Mosaic warts consist of clusters of small warts.
- Benign condylomata (genital warts) are caused by HPV-6 and 11. Classical genital warts are multiple, pointed, and fissured. In women they occur most commonly at the posterior introitus and adjacent labia; also the vulva, perineum, vaginal wall and cervix (a smear should be taken). Warts enlarge during pregnancy and may occasionally obstruct the vagina. In men warts may occur on the frenum, coronal sulcus or glans. Intrameatal warts may spread into the urethra. Perianal warts may spread into the anal canal. They can occur in both homosexual and heterosexual men. HPV 16 +18 appear to risk factors for genital malignancy, and are found in approximately a third of malignancies. However, note that direct transformation from wart to malignancy appears to be very rare. HPV can also be found in cells from a normal cervix. In the UK a recently introduced vaccination programme for 13+ year old girls is aiming to reduce cervical cancer rates by prevention of HPV infection.

Treatment
Most will resolve spontaneously. Genital warts regress less frequently than skin warts.
There are a wide variety of treatments for warts as below. The best evidence base exist for either salicylic acid or cryotherapy. I often try and persuade patients to do nothing if possible!!
- Salicylic acid 20-40% is effective when applied as a paint or plaster after soaking the skin for 5 mins with warm water. The surrounding skin should be protected with a ring of vaseline
- Cryotherapy may be used without anaesthesia but is often not practical for large warts.
- Formalin 10% can be used as a soak for multiple warts on the soles of the feet.
- Fluouracil 5% cream or solution (Efudix®) may be used either alone or alternating with topical retinoids in the treatment of plane warts.
- Podophyllin 10-20% in liquid paraffin may be painted onto anogenital warts and the area then powdered. The coating may be washed off 3-4 hours later. The treatment is repeated 1-3 weekly. It can be irritant and should not be used in pregnancy due to the risk of systemic absorption and damage to the foetus. It should also not be used on the cervix, because of the risk of neoplastic change. If a local reaction occurs the treatment should be stopped and 1% hydrocortisone applied topically twice daily until the inflammation has resolved. The treatment can then be tried again with caution.
- Imiquimod (5%), an immunomodulator, has recently been introduced for genital warts, and trials are ongoing in cutaneous warts.
- Electrocautery may be used for some types of warts but must be done using local anaesthesia.
- Surgical excision may occasionally be used to remove or debulk extensive warts, especially perianal warts.
- Laser evaporation using a carbon dioxide laser can be used for both mucosal and cutaneous lesions.
- Loop electrosurgical excision procedure (LEEP) uses a heated loop to remove cervical lesions. The lesions is removed intact and can be sent for pathological examination
- There is evidence against using Cimetidine.
Molluscum contagiosum
It is caused by a poxvirus and is transmitted from person-to-person and via close body contact. School children are particularly susceptible. Infection occurs through abrasions of the skin.

Molluscum contagiosum – umbilicated, firm white papules. Note the apparent inflammation and 'impetiginisation' which often heralds spontaneous clearing of lesions
The characteristic lesions are small, smooth pearly-white or flesh coloured umbilicated papules which become dome shaped. They vary in size from 1–5 mm and occur commonly on the face, hands, arms, abdomen, buttocks and genitals. They are rare inside the mouth or on the soles of the feet. They may become confluent along lines of abrasions. They can be transmitted to other areas of the body by autoinoculation.
Clinical tip: Giant molluscum in an adult should alert you to a possible underlying HIV infection
Treatment may be sought for cosmetic reasons, particularly for facial lesions. A proprietary preparation containing 5% potassium hydroxide is available in the UK and may lead to resolution of lesions after 4-6 days.
Mucocutaneous lesions caused by viruses
| Virus | Lesion | Virus shedding? | |
| No Systemic Spread |
Papilloma |
Common wart Plantar wart Genital wart |
Yes |
|
Molluscum Contagiosum |
Smooth umbillicated fleshy papule |
Yes | |
| Orf | Papulovesicular | Yes | |
| Systemic spread |
Herpes simplex Varicella zoster |
Vesicular |
Yes |
|
Coxsackie A |
Vesicular, mouth (herpangina) |
Yes | |
|
Coxsackie A16 |
Vesicular (hand, foot and mouth) |
Yes | |
|
Parvovirus B19 |
Facial maculopapular |
No | |
|
HHV6 |
Exanthem subitum (roseola infantum) |
No | |
|
Measles |
Maculopapular |
No | |
| Rubella |
Maculopapular |
No | |
|
Echoviruses |
FUNGAL DISEASES
Fungal infections are tremendously common in dermatological practice but even so we regularly joke that dermatologists often miss the diagnosis of tinea!!
Essentially two types of pathogens cause trouble on the skin:
- Yeasts e.g. candidiasis and seborrhoeic dermatitis.
- Moulds e.g. ringworm and fungal nail infections
Fungal infections
These can be considered as below:
- Superficial mycoses. Very common e.g. 20% people with tinea unguum/pedis
- Deep mycosis. These are uncommon in the UK but more common in the tropics.
- Systemic mycoses. Rare except in immunocompromised. Candida and malassezia species may be part of the normal flora but can cause disease in susceptible individuals
Candidal infections
There are several species, of which the commonest is candida albicans. These are usually superficial infections which thrive in hot sweaty areas. Typically they cause problems as below:
- vulvovaginal (thrush), oral, intertrigo, balanitis, napkin dermatitis
- risk factors: diabetes, pregnancy, immunosuppression
- treat with topical antifungals, e.g. imidazole e.g. polyenes (e.g. nystatin); can treat with oral imidazoles (e.g. fluconazole) if necessary

Candidal intertrigo- note satellite lesions which can help with diagnosis
Candidal nail infection
Clinically this presents with onycholysis, paronychia, dystrophy. May be seen in patients with Raynauds, Cushings, or in people who immerse the hands in water for prolonged periods. Treatment is with oral imidazoles, and advice regarding hand care and avoiding excess moisture.

Chronic paronychia – candida
Chronic mucocutaneous candidosis is rare familial condition which usually presents in childhood with recurrent oral candida and paronychia,
Clinical Tip- Candida and moulds tend to cause paronychia and a lot of inflammation in the periunguum
Amorolfine may be helpful for topical therapy of candida , although it is not very efficacious generally. Needs to be used for up to 12 months.
Malassezia yeast infections
Malassezia furfur is a normal skin flora, previously called pityrosporum species. It commonly presents with problems especially in atopics and immunosuppressed. There are various patterns of infection:
- Seborrhoeic dermatitis – scaling of scalp and face ‘T’ zone-characteristically orange -red hue. Also caused napkin dermatitis.
- Pityriasis versicolor –see below
- Pityrosporum folliculitis – itchy, back and upper trunk in young males- see above.
Pityriasis versicolor
This is a very common rash usually seen in teenagers. Patients usually complain about it when they come back from a holiday and find that the rash is more noticeable when as it didn't tan! Typically we see coalescent orange- brown patches with surface scaling which can be helpful when making the diagnosis. Woods lamp shows pale yellow fluorescence though in reality one doesn't need to use this to make a diagnosis. Slight hyperkeratosis causes brownish colour in white skin, whereas the azaleic acid produced by the yeast causes hypopigmentation in dark skin. Hence the name- versicolor (variable colour).

Pityriasis versicolor – oval hyperpigmented patches
Treatment is with topical antifungals e.g. selenium sulphide (Selsun®) shampoo e.g. ketoconazole (Nizoral®) shampoo or cream e.g. terbinafine (Lamisil®). Occasionally I prescribe oral imidazoles e.g. itraconazole (NOT ORAL TERBINAFINE) if severe or resistant disease. Hypopigmentation persists for months and may become more obvious with a subsequent tan. Warn patients about this!!
Clinical tip: Flaking on scratching the lesions helps confirm the diagnosis
DISEASES CAUSED BY MOULDS
Moulds represent a large group of organisms, most of which are non-pathogenic. Human disease is caused by both dermatophytes and the non-dermatophytes
Dermatophytes = ringworm. There are 3 groups: trichophyton, microsporum and epidermophyton.
Non-dermatophytes = many types of less importance.
Presentation
These are classified according to body part affected e.g. Tinea corporis, tinea capitis, tinea cruris, tinea pedis, tinea unguium. Infection may cross anatomical boundaries, and features are related to the degree of inflammation, which in turn depends on the dermatophyte species e.g. animal species more inflammatory than ‘human’ species.

Tinea cruris – note the well-defined, inflammatory, red edge
Top Tip: Tinea in feet may be a portal of entry for cellulitis
Key features of fungal skin infection
- Well defined lesions that may have a raised edge.
- Single or unilateral.
- May have some vesicles or pustules.
- May look psoriasiform on legs and feet.
- Differentials include discoid eczema, pityriasis rosea with herald patch, lichen simplex, erythrasma.
- May be modified by steroids i.e. tinea incognito
Diagnosis is by skin scrapings for mycological culture or if available with KOH preparations in the clinic.
Treatment- small areas may be treated with topical terbinafine or ketoconazole for 2-4 weeks. In severe or widespread infection or tinea manuum use oral terbinafine or oral itraconazole for 2-4 weeks or longer for toenails - 3 months.Oral itraconazole can be used as a pulsed regime .

Tinea corporis on the arm – note the well-defined leading edge
Performing skin scrapings
- Disposable scalpel or blade which is held perpendicular to skin surface
- Use Firm strokes over edge of lesion without lacerating skin
- Scrape onto black paper (easier to see).
- Fold and seal for transport.

Dermapak envelope for transporting skin scrapings, nail clippings or hair for mycological analysis
Tinea capitis
This is a condition which is more common in children than adults and is much more common in Afro-Caribbean children. There are two common patterns, but it may be very varied in its presentation, from subtle scaling to broken 'black-dot' hairs.
It may cause a patchy rather moth-eaten alopecia –with well defined round areas of hair loss, minimal scale and broken hairs

Tinea capitis – patchy alopecia and scale
Tips: Hair plucks as well as scrapings should be taken. It is painless to extract hairs.
Kerion occurs due to exaggerated host response to presence of mould. Clinically we see a boggy inflamed mass, with pus, matted loose hair & scale crust and sometime associated with lymphadenopathy.
Tip: do not let the surgeons Incise and drain this- it responds to medical treatment, often with full hair regrowth (surprisingly).

Kerion – boggy inflammatory mass with alopecia
Investigation - with scrapings & plucked hair. Woods lamp limited value – only picks up some species.
Treatment -
- griseofulvin 10-20 mg/kg for 2 months has historically been used as first line but more recently many clinicians are using terbinafine half adult dose for 4 weeks as first line therapy. Ketoconazole shampoo should be used for both patient and unaffected siblings and other family members as fomite spread is a major issue with tinea capitis. Children should not need to be excluded from school for this, and it is important to warn of the possibility of an Id reaction, which occurs when treatment of inflamed dermatophyte e.g. kerion results in distant reaction. There are 2 patterns, namely a pompholyx like reaction and follicular papules on trunk and limbs. This resolves with treatment of dermatophyte infection.
Tinea unguium
There is often associated tinea pedis or tinea manuum, therefore take skin scraping as well as nail clippings. There may sometimes just be a couple of nails involved.
Tip: If all nails are affected it is less likely to be tinea and more likely to be primary nail pathology such as psoriasis
There 3 types typically described.
1. distal and lateral subungual onychomycosis (DLSO). This is the most common pattern with yellow/brown/black colour and soft subungual hyperkeratosis. It spreads proximally and other nails may be sub clinically infected. It may cause discomfort.

Extensive Tinea Unguium toe nails
2. white superficial onychomycosis (WSO). This produces powdery white discoloration of the distal nail and is more common in HIV disease but is also found in health adults and children.
3. proximal subungual onychomycosis (PSO) rare except in HIV. Proximal nailfold infection with rapid invasion and white nail without thickening.
Tip: It is worth sending clippings and subungual debris for microbiology. When moulds are involved one sees periungual inflammation
Treatment: terbinafine 250 mg daily for 6 weeks in fingernails and 12 weeks in toenails, or itraconazole pulse 400 mg/day (as 200 mg bd) for 1 week per month for 3-6 months or as 200 mg daily for 12 weeks. It has a long half life and may persist in the nail plate for up to 6 months and may cause taste disturbance which can be permanent. It has minimal drug interactions. It is better for diabetic patients and those with HIV.
Itraconazole is fungistatic but is more broad spectrum and reasonably good for candida and moulds. Pulse therapy is useful as it decreases the risk of toxicity. Monitor LFT if long term or other hepatotoxic drugs.
If treatment is unsuccessful, reconsider diagnosis e.g. trauma, psoriasis, LP, eczema.
Elderly and patients with e.g. psoriatic nails are harder to treat.
Dermatol Ther. 2017 Jan 18. doi: 10.1111/dth.12457. This study looked at efficacy and tolerability of amorolfine 5% nail lacquer in combination with systemic antifungal agents for onychomycosis:
The efficacy and safety of amorolfine 5% nail lacquer in combination with systemic antifungal agents in the treatment of the onychomycosis were evaluated. According to meta-analysis, combination treatment of amorolfine 5% nail lacquer and systemic antifungals can result in higher percentage of complete clearance of onychomycosis. It showed that the experimental combination group was more effective than monotherapy of the systemic antifungals [OR (odds ratio) = 1.97, 95%CI (95% confidence interval) = 1.44-2.69], and no more adverse events happened with the addition of amorolfine 5% nail lacquer (OR = .96, 95%CI = .56-1.63, p = .95). This effect strengthens the fact that amorolfine 5% nail lacquer in combination with systemic antifungal agents was better than the monotherapy of systemic antifungals like itraconazole and terbinafine.
Non-dermatophyte mould infections
These are relatively uncommon in the UK but more common in some tropical countries, USA and the Mediterranean region. e.g. Scytalidium spp:
-
Causes Ringworm like infections
-
Affects palms, soles and webspaces
-
Nails are frequently involved, including onychomycosis
-
It is difficult to treat with usual oral antifungals
-
It may require nail removal.
-
Whitfield’s ointment can be useful for scaling sole lesions
Other fungal infections
The rest of the fungal infections are mostly subcutaneous or systemic and tend to occur in Indian subcontinent, Middle-East and Africa
Subcutaneous mycoses
These are infections caused by fungi which are directly inoculated into the dermis or subcutaneous tissue through a penetrating injury. Mainly seen in the tropics.
Sporotrichosis
Fungus is usually introduced by trauma, e.g. by a thorn or splinter, usually into the upper limb where a nodule or pustule forms and via lymphangitic spread a chain of nodules develops. Whilst it may resolve spontaneously it is usually treated with Itraconazole.

Systemic mycoses
These are fungal infections that involve deep structures and can spread, usually via the bloodstream, to a site distant from the original focus of infection.
Cryptococcus yeast in HIV infection

- Often resembles molluscum contagiosum on the skin
- Systemic involvement is usual – CNS and lungs
- Needs amphotericin B + imidazoles
COMMON PARASITIC INFECTIONS
Scabies
This is one of the most itchy rashes around. Diagnostic clues include
- interdigital, penile, peri-umbilical, flexures, axillae
- contact history
- crusted scabies in immobile/immunosuppressed
Clinical Tip: Itch is often out of proportion to what you see on skin - there may not be many obvious burrows etc.
Clinical Tip: nodules on the shaft of the penis are pathognomic for scabies.


Scabies – note linear burrows at typical site of wrist. Feet are commonly involved in children.

Crusted scabies – loads of mites!

Scabetic nodules – commonly seen in genital region

Scabies mite – isolated with needle
Treatment
Scabies - patient Information Leaflet
The Key to Success is to treat both the patient and all close contacts at the same time with two treatments a week apart, using topical Permethrin 5% cream, applied from the neck down and washed off after 12 hours, reapplying if hands are washed.
Ivermectin orally is needed for immunosuppressed or crusted scabies.
Apologies that we have covered so much this week - and even then there are a number of common infections which we have not had the opportunity to cover in depth. HIV infection will be covered later in the course.
KEY LEARNING POINTS COMMON INFECTIONS.
1. Staphylococal infections are common causes of skin disease and range from impetigo and folliculitis to staphylococcal shock syndromes.
2. Any annular lesions think of Tinea and look for tinea elsewhere e.g. nails, interdigital spaces.
3. Any itchy patient think scabies!! Remember to treat both the index case and all close contacts at the same time and repeat one week later.
4. Any purpuric rash or vasculitis remember Meningococcus.
5. Wart treatment can be complicated and time consuming and ensure the treatments are not more burdensome than the condition.
MODULE 1 – Week 3
Introduction and Common Dermatological Problems - Common Skin Infections
pplementary Material
Please see the BAD website for Patient Information Leaflets on Boils, Chronic Paronychia, Erysipelas, Fungal infections of the nail, Impetigo, Molluscum Contagiosum, Pityriasis Versicolor, Scabies and Shingles
- Necrotizing Fasciitis
- Pediculosis and Scabies A Treatment Update
- Superficial Fungal Infections
- Diagnosis and Management of Necrotising Fasciitis
- Top 10 Tips Tinea Pedis
- BAD Guidelines Onychomycosis
- BAD Guidelines Tinea Capitis
- Practice Guidelines for the Diagnosis of Skin and Soft Tissue Infections
- Cellulitis CREST guideline
- Diagnosis and management of cellulitis
- Dermatophytosis the Management of Fungal Infections
- Infected skin ulcer
- Ectoparasite in Travelers
- HSV labialis
- HSV
- Scabies intervention cochrane review
- Malassezia (p69-71)
- Chronic wound & antibiotics
- Mx of common Skin infection
- BAD - Guidelines for treatment of onychomycosis
- Psoriasis or scabies
- Scabies wake sign
- Tinea Vesicolor
- Mx Molluscum Cochrane Review
- Necrotising fasciitis
- Common skin infections in children
- BAD Cutaneous Warts Guidelines
MODULE 1 – Week 3
Introduction and Common Dermatological Problems - Common Skin Infections
Multimedia Resources
- Tinea Imbricata (video)
- Tinea Corporis (video)
- Herpes Zoster (video)
- Bacterial skin infection 1 - Interview with Dr David Paige (audio)
- Bacterial skin infection 2 - Interview with Dr David Paige (audio)
- Viral skin infection 1 - Interview with Prof Judy Breuer (audio)
- Viral skin infection 2 - Interview with Prof Judy Breuer (audio)
- Fungal, parasitic and mycobacterial skin infections 1 - Interview with Dr A Sohota (audio)
- fungal, parasitic and mycobacterial skin infections 2 - Interview with Dr A Sohota (audio)
- Granulomatous (video) ***NEW***